Cold water immersion (a.k.a., “ice baths”) has become a popular method amongst exercise enthusiasts and athletes to enhance recovery after an intense training bout. The strategy involves exposing either the trained limb or the whole body to very cold liquid temperatures. According to p...
Brad Schoenfeld, Ph.D, C.S.C.S., is an internationally renowned fitness expert and widely regarded as one of the leading authorities on body composition training (muscle development and fat loss). He is a lifetime drug-free bodybuilder, and has won numerous natural bodybuilding titles.
The beauty of science is that is self-correcting. When a study is published, others get to scrutinize the data and methods. When issues arise, the scientific community gets to discuss and debate the findings, and when appropriate, challenge their veracity.
Recently, I collaborated with some of the world’s top sports scientists on a letter to the editor about a study published in the Journal of Strength and Conditioning Research, that showed an extremely large anabolic effect to consuming a supplement containing HMB+ATP. We wrote an extensive letter that covered our issues with the paper in hopes of seeking truth in science. However, we had to substantially cut down our response to conform to the journal’s policy of allowed only 400 words in such letters. This watered down our points so that the true impact was markedly diminished.
Thus, I wanted to present the unedited version of our letter here so that further discussion can be had on the topic. Only through discourse can we maintain confidence in the research process and facilitate true evidence-based practice.
Extraordinary changes in body composition and performance with supplemental HMB-FA+ATP
Stuart M. Phillips, Ph.D., McMaster University
Alan Aragon, M.S., California State University, Northridge
Shawn M. Arent, Ph.D., Rutgers University
Graeme L. Close, Ph.D., Liverpool John Moores University
D. Lee Hamilton, Ph.D., University of Stirling
Eric R. Helms, M.S., M.Phil, Sports Performance Research Institute New Zealand
Jeremy P. Loenneke, Ph.D., The University of Mississippi
Layne Norton, Ph.D., Owner BioLayne LLC
Michael J. Ormsbee, Ph.D., Florida State University
Craig Sale, Ph.D., Nottingham-Trent University
Brad J. Schoenfeld, Ph.D., Lehman College
Abbie Smith-Ryan Ph.D., University of North Carolina
Kevin D. Tipton, Ph.D., University of Stirling
Matthew D. Vukovich, Ph.D., South Dakota State University
Colin Wilborn, Ph.D., University of Mary Hardin-Baylor
Darryn Willoughby, Ph.D. Baylor University
The authors of this letter read with skepticism the recent report from Lowery et al. (10), employing a supplement that provided 3g of beta-hydroxy-beta-methyl butyrate as a free acid (HMB-FA; three doses of 1g each) plus 400mg of oral adenosine triphosphate (ATP) in young men who resistance-trained for 12wk. Lowery et al. (10) report gains in lean mass and performance that are greater than those reported in a similarly surprising earlier study from Wilson et al. (18). Our skepticism of the results reported by Lowery et al. (10) exists on several levels. However, our collective disbelief of these data rests on the collective experience of the authors of this letter, who have conducted more than 60 resistance training studies, and who have never observed gains in lean body mass that are of a similar incredibly uniform magnitude as those reported by Lowery et al. (10). As opposed to the often-observed heterogeneity in resistance training-induced hypertrophy, Lowery et al. (10) must have observed remarkably consistent between-group changes in muscle mass to find statistical significance between the supplemented and placebo groups. What makes this more remarkable in that this was seen in a total of 17 subjects (n=9 placebo, n=8 HMB-FA+ATP). We are particularly nonplussed on this point since the sharp ‘divergence’ between the HMB-FA+ATP versus placebo groups occurred in the face of what the authors refer to as an optimal training paradigm, with optimal nutritional support, and the advice of an experienced dietitian. And thus the difference is due, ostensibly, to two compounds (HMB-FA and/or ATP), which have been studied previously and resulted in a trivial training-induced adaptive advantage (13). Would the authors be willing to share subjects’ individual data? We ask since the mean gain in lean body mass in the supplemented group was ~8.5kg (10), meaning there had to be some subjects who gained more and uniformly so for the treatments (in only 17 subjects) to be so robustly different! This is also an astounding gain of lean body mass when one considers that the subjects were previously resistance-trained and so would have had less propensity to gain lean body mass (11). We could not ascertain the absolute values for the beginning and final values for body composition and so readers would have to make assumptions (since the reported data were incomplete and given as percentages) as to how much body composition changed. Would the authors be willing to present these data?
We are aware of a previous letter from Hyde et al. (7) asking for clarification from Lowery et al. (10) on their methods. Thus, our concern is clearly shared by others and, given the number and research experience of the authors on this letter, quite widespread. In their reply to this letter (7) Lowery et al. (10) went to great lengths to compare their rates of hypertrophy with those previous reported by other studies. Importantly, however, a number of studies discussed by Lowery et al. (10) as having comparable ‘rates’ of hypertrophy were markedly (5wk) shorter than their 12wk intervention (14). Thus, while ‘rates of hypertrophy’ (assessed with different methods and in different labs (3, 9, 14, 16), in different study populations, being overfed and not exercising (3), with different dietary backgrounds (3, 9, 14, 16), and/or consuming different supplements (i.e., creatine) (9, 14, 16), may have been similar (or greater) to those seen by Lowery et al. (10) the total accrued (over 12wk) lean body mass cannot be assumed to be linear and extrapolated to that seen in their study. Further, what is revealing is the astonishing performance differences reported by Lowery et al. (10), which implies not only greater total lean mass gains but an extraordinary functionality to the accrued lean mass or by some other unexplained mechanism. That is, why did HMB-FA+ATP impart an astonishing ‘functional overreaching’ response with the optimal training paradigm, with great dietary support, and in highly trained and motivated subjects and not in the placebo group?
It is important to understand the limitations of dual-energy x-ray absorptiometry (DXA), which derives by difference fat- and bone-free mass, which is a variable that is not equivalent to muscle (6, 12). The limitations of DXA and ultrasound, the two muscle-based outcome measures have been clearly outlined in a recent review (6). As stated, DXA “Cannot specifically discern skeletal muscle mass [bold added] and quality as can CT [computerized tomography] and MRI [magnetic resonance imaging]” and is subject to changes in hydration status (6). For ultrasound, “Technical skill required. Excess transducer pressure and orientation can influence muscle size measurements. Identification of reproducible measurement sites critical. Care needed to make sure muscle is in relaxed state. Conditions such as proximity to exercise bout, hydration, are important to control” (6). Lowery et al. (10) report nothing with respect to the ultrasound machine used, the hydration or feeding status of their subjects, or proximity to an exercise. It would be useful for readers if Lowery et al. (10) would detail for the readers the training level of the researcher(s) who conducted the ultrasound tests (inter-rater reliability of more than one researcher was used), noted whether more than one researcher carried out testing, whether these testers were blinded to the group assignment while completing/analyzing the thickness measures, and clarify the temporal aspects of testing to determine if there may be any associated confounding issues.
In the response to Hyde et al (7) Lowery et al. (10) purport to have selected “…a responsive population who possess a quantity of lean mass indicative of previous responses to resistance training…” Notwithstanding the scientific inaccuracy of this statement, the authors must have gone through a screening process of sorts to recruit 17 subjects with lean mass “…an order of magnitude [we note that an order of magnitude is defined as 10-times greater so this cannot be the case] higher than average lean mass typically seen in recreationally trained subjects…” Could the authors please state what the exact criteria for inclusion as a subject in this study were? Can the authors please detail the screening process describing how many subjects were recruited and screened, final entered the study, and dropouts, to reach this number of subjects meeting these criteria and who completed the protocol? Please also clarify if the subjects were randomised to treatment and placebo groups or pair matched based on body mass, lean body mass, strength or other variable.
The only form of HMB for which there is plausible data showing a mechanistic underpinning for its potential role aiding in muscle protein turnover is for calcium-HMB (15). We are unaware of any similar proof-of-principle mechanistic data for the free acid form of HMB despite apparently greater bioavailability and uptake (into what tissue is unclear) (4). Do the authors know of any data showing that HMB-FA has a similar credible effect as calcium-HMB on human muscle protein turnover (15)? We note that leucine had the same anabolic effects as calcium-HMB (15). We also note that dietary protein can exert a positive effect on gains in muscle mass with resistance training (1) and yet the placebo group did not appear to respond at all to the overreaching phase. As another ingredient of the supplement used by Lowery et al (10), ATP would appear to be, given an extraordinarily low bioavailability (2), to be unusable. However, we note that Wilson et al. (17), using the same study protocol as that employed by Lowery et al. (10), reported that ATP (400mg/d) resulted in a positive effect on muscle mass, strength, and power gains. This seems to us highly improbable given that oral ATP even up to doses of 5000mg/d [more than an order of magnitude greater than the dose used by Wilson et al. (17) and Lowery et al. (10)] for 4wk leads only to increases in circulating uric acid with no detectable changes in ATP in the blood (2) let alone muscle. Thus, as opposed to an inconsequential increase in post-exercise blood flow induced by the ATP (8) in the HMB-FA+ATP supplemented group, we find it biologically implausible that 400mg/d of oral ATP would exert any effect on processes leading to enhanced performance let alone hypertrophy. What is remarkable is that given the expert dietary advice and total protein intake of the subjects studied, the optimal training program, and ‘responsive’ subjects that the differences in lean mass (and performance) between the HMB-FA+ATP and placebo groups are as impressive as they are (10). Moreover, that these differences are statistically significant in such a small sample of subjects and ascribed to an, as yet, mechanistically untested form of HMB and a biologically unavailable quantity of ATP.
We ask, in accordance with all reasonable guidelines regarding full disclosure of potential conflicts of interest now in place at many journals (including the Journal of Strength and Conditioning Research – http://journals.lww.com/nsca-jscr/Pages/InstructionsforAuthors.aspx – accessed Oct 1, 2016) that Dr. Wilson and Mr. Lowery disclose here whether they have ever received travel expenses, stipends, or honoraria, or shares associated with their work and the companies involved with ATP and/or HMB and/or whether they or their spouses have any public or private interests with Metabolic Technologies, Inc. and/or companies selling or dealing in oral ATP supplements or their affiliates? This is not an accusation and we fully accept that neither Dr. Wilson nor Mr. Lowery may have ever received such support, but believe this is an honest and reasonable question to ask on both scientific and ethical grounds (5) and it is standard practice to make such disclosures.
Reference List
1. Cermak NM, Res PT, de Groot LC, Saris WH and van Loon LJ. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: a meta-analysis. Am J Clin Nutr 96: 1454-1464, 2012.
2. Coolen EJ, Arts IC, Bekers O, Vervaet C, Bast A and Dagnelie PC. Oral bioavailability of ATP after prolonged administration. Br J Nutr 105: 357-366, 2011.
3. Forbes GB, Brown MR, Welle SL and Lipinski BA. Deliberate overfeeding in women and men: energy cost and composition of the weight gain. Br J Nutr 56: 1-9, 1986.
4. Fuller JC, Jr., Sharp RL, Angus HF, Baier SM and Rathmacher JA. Free acid gel form of beta-hydroxy-beta-methylbutyrate (HMB) improves HMB clearance from plasma in human subjects compared with the calcium HMB salt. Br J Nutr 105: 367-372, 2011.
5. Gorman DM. Can We Trust Positive Findings of Intervention Research? The Role of Conflict of Interest. Prev Sci 2016.
6. Heymsfield SB, Gonzalez MC, Lu J, Jia G and Zheng J. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc Nutr Soc 74: 355-366, 2015.
7. Hyde PN, Kendall KL and LaFountain RA. Interaction of beta-hydroxy-betmethylbutyrate free acid and adenosine triphosphate on muscle mass, strength, and power, in resistance trianed invidividuals. J Strength Cond Res 30: e10-e14, 2016.
8. Jager R, Roberts MD, Lowery RP, Joy JM, Cruthirds CL, Lockwood CM, Rathmacher JA, Purpura M and Wilson JM. Oral adenosine-5′-triphosphate (ATP) administration increases blood flow following exercise in animals and humans. J Int Soc Sports Nutr 11: 28, 2014.
9. Jowko E, Ostaszewski P, Jank M, Sacharuk J, Zieniewicz A, Wilczak J and Nissen S. Creatine and beta-hydroxy-beta-methylbutyrate (HMB) additively increase lean body mass and muscle strength during a weight-training program. Nutrition 17: 558-566, 2001.
10. Lowery RP, Joy JM, Rathmacher JA, Baier SM, Fuller JC, Jr., Shelley MC, Jager R, Purpura M, Wilson SM and Wilson JM. Interaction of Beta-Hydroxy-Beta-Methylbutyrate Free Acid and Adenosine Triphosphate on Muscle Mass, Strength, and Power in Resistance Trained Individuals. J Strength Cond Res 30: 1843-1854, 2016.
11. Morton RW, Oikawa SY, Wavell CG, Mazara N, McGlory C, Quadrilatero J, Baechler BL, Baker SK and Phillips SM. Neither load nor systemic hormones determine resistance training-mediated hypertrophy or strength gains in resistance-trained young men. J Appl Physiol (1985) 121: 129-138, 2016.
12. Prado CM and Heymsfield SB. Lean tissue imaging: a new era for nutritional assessment and intervention. JPEN J Parenter Enteral Nutr 38: 940-953, 2014.
13. Rowlands DS and Thomson JS. Effects of beta-hydroxy-beta-methylbutyrate supplementation during resistance training on strength, body composition, and muscle damage in trained and untrained young men: a meta-analysis. J Strength Cond Res 23: 836-846, 2009.
14. Stone MH, Sanborn K, Smith LL, O’Bryant HS, Hoke T, Utter AC, Johnson RL, Boros R, Hruby J, Pierce KC, Stone ME and Garner B. Effects of in-season (5 weeks) creatine and pyruvate supplementation on anaerobic performance and body composition in American football players. Int J Sport Nutr 9: 146-165, 1999.
15. Wilkinson DJ, Hossain T, Hill DS, Phillips BE, Crossland H, Williams J, Loughna P, Churchward-Venne TA, Breen L, Phillips SM, Etheridge T, Rathmacher JA, Smith K, Szewczyk NJ and Atherton PJ. Effects of leucine and its metabolite beta-hydroxy-beta-methylbutyrate on human skeletal muscle protein metabolism. J Physiol 591: 2911-2923, 2013.
16. Willoughby DS, Stout JR and Wilborn CD. Effects of resistance training and protein plus amino acid supplementation on muscle anabolism, mass, and strength. Amino Acids 32: 467-477, 2007.
17. Wilson JM, Joy JM, Lowery RP, Roberts MD, Lockwood CM, Manninen AH, Fuller JC, De Souza EO, Baier SM, Wilson SM and Rathmacher JA. Effects of oral adenosine-5′-triphosphate supplementation on athletic performance, skeletal muscle hypertrophy and recovery in resistance-trained men. Nutr Metab (Lond) 10: 57, 2013.
18. Wilson JM, Lowery RP, Joy JM, Andersen JC, Wilson SM, Stout JR, Duncan N, Fuller JC, Baier SM, Naimo MA and Rathmacher J. The effects of 12 weeks of beta-hydroxy-beta-methylbutyrate free acid supplementation on muscle mass, strength, and power in resistance-trained individuals: a randomized, double-blind, placebo-controlled study. Eur J Appl Physiol 114: 1217-1227, 2014.
We are glad that more and more people are demanding and applying evidence in the exercise and nutrition field. That been said, there remains a lot of misunderstanding and misconceptions about an evidence-based Practice (EBP). In this article, we will address some of the common misconceptions and criticisms of EBP. Here we go:
Why do we need EBP? Why can’t we just use anecdotal evidence or expert opinion?
In fact, we’ve used anecdote or expert opinion as ‘evidence’ to treat people throughout the history of medicine. But this approach clearly didn’t work well as shown by hundreds of examples of medical mistakes we made in the past. For example, smoking was ‘good’ for heath until studies showed otherwise; bloodletting was the standard medical treatment for almost 2000 years by the foremost doctors of the West, and so forth. In short, EBP evolved because anecdotal evidence or expert opinion were not producing ‘results’.
The definition of EBM (Evidence Based Medicine) by David Sackett reads: “EBM is a systematic approach to clinical problem-solving that allows integration of the best available research evidence with clinical expertise and patient values”. This principle can be applied across many scientific disciplines, including exercise and nutrition, to optimize results.
What is the evidence?
Many people wrongly assume that the term “best available evidence” in EBM/EBP is limited to research-based evidence. In fact, evidence can be obtained from a well conducted randomized controlled trial, an unsystematic clinical observation, or even expert opinion. For example, the evidence could come from a controlled trial, your favorite fitness guru, or a physiological mechanism. However, the critical point is that the importance or trust we place on the evidence differs based on the type of evidence. We will talk more about this as we talk about the evidence hierarchy.
What about values and preferences?
Every patient or client assigns his/her own values, preferences, and expectations on outcomes and decisions.
For example, some might place a high value on muscle growth, whereas others would value their general health as most important. Some would value building their upper body muscles more than their lower body muscles. Others may value the social aspect of working out at a gym more than the muscle and strength gains.
And rightly so, these personal decisions have no wrong or right and should be listened to and respected. The job of a fitness professional is to help clients achieve whatever goals they desire; we cannot impose our own values no matter how contrasting beliefs and opinions maybe.
What about clinical expertise? And what is the ‘art’ of EBP that people always talk about?
Clinical expertise is what many refer to as the art of EBP. So, does the art of EBP mean applying what has worked for your clients? Clearly not.
Clinical expertise involves basic scientific knowledge, practical expertise, and intuition to:
• diagnose the problem (for example, why can’t this person squat deep, how to correct exercise technique, why he/she is not gaining strength or losing weight.),
• search for the relevant research evidence (how many sets to gain muscle for an advanced trainee, or which exercise targets specific muscles) and critically analyze the research evidence for methodological issues (was the study in beginners, was the outcome measured relevant)
• understand both the benefits, the risks involved, and other alternative approaches to the goal (a Crossfit type workout might be motivating and improve general cardiovascular endurance, but has a high risk of injuries)
• alter the program based on the client feedback and results (reducing the number of sets or modifying the exercise (angles, ROM and do forth) for an older person or someone with pre-existing shoulder injuries.)
• Listen and understand clients value and preferences, clearly communicate the risk, cost, benefits in a simple manner, and use a shared decision approach to come to a decision
And this is called the art of evidence-based approach. As you can see, it forms an integral part of EBP and no amount of research can replace it. Likewise, no amount of clinical expertise can replace research evidence.
What is the evidence hierarchy? And why are RCT’s (Randomized Clinical Trial) at the top of the pyramid?
An evidence hierarchy is one of the foundational concepts of EBP. And there are three important points to keep in mind:
• First, as shown, the different types of evidence are arranged in an orderly fashion. As we go up the hierarchy, the trust or the confidence we place in the study results go up too. RCT’s are the most valid research design, as they allow the ability to infer causality. And expert evidence is the least trustworthy and occupies the bottom position. Meta-analyses- a collection or a group of RCT’s-are generally considered the highest form of evidence, as they synthesize the entire body of literature on a given topic and quantify the results based on a statistical measure of practical meaningfulness. Meta-analyses can be particularly important in exercise- and nutrition-related topics, as the sample sizes are often small and thus pooling the data across studies provides greater statistical power for inference.
• Second, it is important to note that depending on the quality of the study, an RCT can be downgraded, too. A poorly designed study will never provide a high level of evidence, and in fact can impair the ability to draw proper evidence-based conclusions. The hierarchy therefore is not set in stone.
• Third, there is always evidence. So the best available evidence is what is available and need not come from an RCT (Randomized Controlled Trial). But based on the type of evidence, our confidence in the results and our recommendations will differ accordingly.
What if there are no RCT’s? How do I evaluate a program or diet?
First, as mentioned before, there is always evidence. If there are no RCT’s, you simply move down the evidence hierarchy. But as you go lower in the hierarchy, uncertainty about the validity of the evidence goes up as well. Second, you also must compare the benefits, risks, cost, scientific plausibility, and other alternative programs before making recommendations. Below are a few examples where the absence of an RCT does not preclude recommendations.
Example 1: If a client comes with a new program that uses 5 lb weights to increase strength, we know from basic science that without load progression, muscle and strength gains will be nil. Such a program would go against the most fundamental theory of muscle growth. So you can make a strong recommendation against the program, even without an RCT.
Example 2: Recently, the Ebola virus vaccine was used before conducting an RCT. How is that possible? Here is a classic example of weighing the benefits, risks, alternative approaches, and making a strong recommendation with weak evidence. In this case the risk is death, the benefit is obvious, and there are no alternative approaches. Thus, the risk/reward strongly favored giving the vaccine. And 99% of the informed patients would agree with the recommendation.
Example 3: If a client wants to try the Xfit program, you can convey the lack of studies (weak evidence), the risks involved, the time required for learning the right technique, and give other programs which are in line with her/his goals. If he/she still wants to do it, he/she shouldn’t be critiqued for their decision.
Example 4: An observational study shows that eating meat raises cancer. Considering observational studies are lower in the hierarchy no matter how well the study is conducted, recommendations cannot be more than just suggestions.
What if there are no studies and my client wants to try a new program?
As previously noted, if a person understands the uncertainty due to the lack of studies or weak evidence, availability of alternative programs that fit his/her goal, the cost, and risks, he/she can make an informed personal choice. Keep in mind that majority of the questions in exercise and nutrition are of weak evidence. In fact, it is the same for the medical field too. But what is important is to clearly know and convey what your recommendations are based on.
There are a lot of factors like genetics, diet, motivation that can influence your results. A study hence…
Many people are unaware that in a randomized controlled trial, the randomization serves a crucial purpose: The randomization ensures, at least theoretically, that both the known variables and unknown variables that can affect muscle growth or strength are equally distributed into both groups. That is, if there are unknown genetical factors that can drive muscle growth, it is highly likely these genetically gifted individuals will be distributed evenly. This is the reason why RCT are considered to be the gold standard to study cause and effect. Hence, the results of the study can be pinned to the intervention or treatment
There are numerous problems with scientific study. So you cannot use the results of a study to train your clients?
Yes. But one of the basic steps in EBP is to critically analyze the study: If the study has methodological issues or has a different population than your client, you downgrade the evidence accordingly and lower your strength of recommendations.
Most of the studies in bodybuilding/strength training are on untrained individuals.
Yes. And rightly so, caution should be used when extrapolating recommandations to trained individuals. Exercise science is a relatively new field and studies in trained individuals are small in number, but accumulating. Generalizability (i.e. the ability to apply findings from a study to a given population) must always be taken into account when using research to guide decision-making.
I don’t care about “why” it works or the science behind. All I care about are results.
As previously mentioned, EBP evolved to get better results. It didn’t evolve to explain how or why a treatment works. There are 1000’s of life saving treatments and drugs where the underlying mechanism(s) are just unknown.
Studies are looking at an average of the sample. There is a lot of individual differences.
Yes. In fact, n=1 studies occupy the top of the evidence hierarchy because it applies to the specific individual in question. But these are hard and almost impossible for certain outcomes like muscle growth or disease prevention. There are two concerns with so-called trial and error method that is often talked about.
• First, even if you gain benefits with a certain program, in many cases, it is extremely hard to figure out what was the variable that made the difference. Was it the specific exercise, the change in diet, the placebo effects, genetics, or some unknown variable?
• Second, it may not be clear if you are indeed making an improvement depending on the outcome. For example, gains in muscle come very slowly for trained individuals (like years for a several pounds). Hence, you will have to run a program for a few years to see if it works or not. However, controlled research often uses measures that are highly sensitive to subtle changes in muscle mass, and thus can detect improvements in a matter of weeks.
The program worked for me!
What was the outcome measure? Strength, muscle growth, weight loss? What are you comparing against? Against your previous results? What was the magnitude of the benefit? Without knowing answers to these questions, the meaning of the word ‘worked’ is unclear.
Further, if it indeed worked, we still don’t know what made it work, or if it will work for someone else. So your personal anecdotes are often fraught with problems and unfortunately mean very little. And importantly, just because something “worked” doesn’t mean that another approach might not work better.
This X supplement was shown to increase muscle growth in an animal study. Should I use it?
Research in animal models is almost at the bottom of the evidence hierarchy. It is very weak and hence the uncertainty is high, and deserves no greater than a weak recommendation. Although animal models can serve an important purpose in preliminary research, evidence based practice should rely primarily on human studies when developing applied guidelines.
A lot of the research is sponsored by nutritional and exercise machine companies. Hence not trustworthy.
Yes. If there is a conflict of interest, the study is downgraded.
I saw a supplement study which showed a statistically significant weight loss. Can I use that supplement for my client?
No, you also have to look at how much weight the subjects lost. The term “significance” is a function of the probability of results occurring by random chance; it is not necessarily related to the magnitude of the effect. Provided a large enough sample size, results of a study can be statistically significant even with just a 1 lb weight loss over a 1 year period. This is known as ‘clinical significance’.
Would you take a supplement to lose 1 lb in a year? Depending on the cost, the burden of taking a pill every day, and how much you value weight loss, you may or may not.
EBP does not consider a science-based approach.
EBP does consider a science-based approach. A science-based approach provides strong evidence when the program or treatment violates fundamental principles or universal laws. For example, homeopathy.
However, EBP does not support evidence just based on biological plausibility or mechanistic evidence. For example, if a new diet tells you to eat as much as you want to lose weight, it goes against fundamental laws of thermodynamics. You do not need an RCT to make strong recommendations against this diet
“This house believes that in the absence of research evidence, an intervention should not be used” This was the motion of a debate which took place at the end of the recent PhysioUK2015 Conference in Liverpool.
As you know by now, EBP does not exclusively rely on RCT’s. To quote the famous saying in EBP: “There is always evidence”. It is an unfortunate misrepresentation of EBP/EBM to assume that without RCT’s, a treatment cannot be recommended. For example, smoking has perhaps the greatest detrimental effect on health of any social habit, and health-based organizations universally recommended against its use. But we do not even have even a single RCT on smoking!
Effects of smoking are from observational studies. But since the magnitude of harm is very high, it upgraded in the evidence pyramid. Once again, this shows why the hierarchy is not set in stone.
‘Parachute use to prevent death and major trauma related to gravitational challenge’. This is the title of the paper published in BMJ. The paper satirically argues that parachute use has not been subjected to rigorous evaluation by using RCTs’ and therefore has not been shown to save lives. Critics of EBP have used this as a criticism of EBP and the reliance of RCT’s.
EBP has always maintained that RCT’s are not required when the magnitude of benefits is very high.
For example, insulin injection for diabetes, Heimlich maneuver, and anesthesia are all examples of treatments where the magnitude of benefit is very high, and hence RCT’s are not required nor asked for.
I do not have enough knowledge to critically analyze studies.
In closing, we hope the article has helped you better appreciate and understand this simple framework called evidence based practice or evidence based medicine. EBP is currently the best approach we have to make decisions related to health, fitness or strength and conditioning. A good EBP practitioner should have a strong understanding of both the practical and the scientific aspects of exercise and nutrition; and more importantly, an untiring commitment and empathy to your clients and their values and preferences.
A popular theory among fitness professionals is that taking short rest periods between sets maximizes muscular growth. The theory is primarily based on the hormone hypothesis, whereby limiting inter-set rest promotes greater elevations in post-exercise growth hormone, IFG-1 and testosterone, and thus enhances the anabolic response to resistance training. One little problem: Emerging evidence indicates that acute increases in anabolic hormones have little if any effect on muscular adaptations, as detailed in my comprehensive review of the topic
In an effort to directly test the theory, our group published a study last year titled, Longer inter-set rest periods enhance muscle strength and hypertrophy in resistance-trained men. In brief, the study not only refuted the claim of a hypertrophic benefit to short rest periods, but in fact showed that resting 3 minutes between sets actually produced superior growth compared to resting 1 minute. Importantly, the study was carried out using a moderate rep range (8-12 reps/set) with all sets performed to muscular failure. The question therefore arises whether results would be applicable when training with lighter weights. No study had ever investigated the topic.
What We Did
Subjects were 21 young collegiate athletes who had not performed resistance training for at least 2 years prior to the study. The subjects were randomly divided into two groups: A short rest group (SHORT) that rested 30 seconds between sets and a long rest group (LONG) that rested 2.5 minutes between groups. The load was set at 40% of the subjects’ 1RM in the back squat and bench press using a tempo of 1-0-2 (1 second on the concentric, 2 seconds on the eccentric). Four sets were performed for each exercise, with all sets taken to muscular failure. Training was carried out twice a week for 8 weeks.
What We Tested
Measures of muscle hypertrophy and strength were assessed pre- and post-study. Muscle cross sectional area (CSA) of the triceps and thigh was measured by MRI. A 1RM bench press and squat was employed to measure changes in maximal strength.
What We Found
With respect to hypertrophy, the SHORT group increased muscle CSA by 9.8% while LONG showed an increase of 10.6%. Thigh CSA increased by 5.7% in SHORT versus 8.3% in LONG. No statistically significant differences were noted between any measure of muscle growth.
From a strength standpoint, 1RM in the bench press increased by 9.9% in SHORT and 6.5% in LONG while increases in the squat were virtually identical between groups (5.2% versus 5.4) As with the hypertrophy results, no statistically significant between-group differences were observed in the strength measures.
How Can You Apply These Findings
There are a number of interesting takeaways from the study. First and foremost, this is yet another study showing that training with light weights can promote marked gains in muscle mass in a relatively short time period. There is now a large body of supporting research on the topic using varied methodologies across a variety of populations. The evidence is too compelling for even the most ardent critic to dismiss.
Intriguingly, we found that rest interval length had no statistically significant effects on muscular adaptations. On the surface, these results conflict with our previous research showing that 3 minutes rest produced superior increases in strength and hypertrophy compared to resting 1 minute when training in a moderate rep range (~10RM). Our findings here seem to indicate that rest interval length isn’t an important consideration when training with lighter loads.
A closer look at the data, however, suggests a more nuanced take-home message.
It’s important to realize that the term “statistical significance” refers to the probability of an event happening by chance. Our study had a fairly small sample size, which reduces the ability to detect significance. Hence, we have to look beyond whether results were “significant” and consider other statistical measures. To that end, while hypertrophy of the arms was fairly equal between conditions, gains in thigh muscle CSA clearly favored resting longer between sets. A statistic called the effect size, which is a gauge of the meaningfulness of the results, bears out these differences were indeed consequential. The effect size for the LONG group was 0.93 (considered a large effect) while that of the SHORT group was just 0.58 (considered a moderate effect). The chart above illustrates the absolute differences between thigh growth and rest intervals.
When attempting to reconcile the differences between upper and lower body hypertrophy, it may well come down to total training volume. Short rest blunted increases in training volume in both upper and lower training, but the disparity was much more pronounced in the squat than in the bench. This is logical as the leg/glute muscles have much greater muscle mass than those of the upper trunk/arms, and thus the associated fatigue during high-rep training is greater in multi-joint lower body training, particularly a demanding exercise like the squat. Given the known dose-response relationship between hypertrophy and volume (as clearly displayed in our recent meta-analysis on the topic), the substantial decrease in number of reps performed with short rest periods could conceivably explain the lesser muscle growth seen in the thighs.
In addition to the long-term effects, we also measured hormonal elevations from each condition post-exercise. Both SHORT and LONG showed significant acute spikes in growth hormone and IGF-1, but the increases were similar between groups. Since hormonal increases are related to levels of metabolic stress, it can be inferred that metabolic stress was similar between conditions as well. Although short rest periods have generally been shown to enhance metabolic stress, these findings are specific to moderate rep training. Training with very high reps elicits large increases in lactic acid regardless of how long you rest between sets. Thus, rest interval length seemingly has less relevance in promoting metabolite buildup. Whether metabolic stress influenced results in this study is undetermined as we didn’t seek to assess mechanisms of adaptations. That’s an intriguing topic for future research.
The Bottom Line
* Training with light weights can pack on some serious muscle.
* Short rest between sets has a detrimental effect on lower body hypertrophy when squatting while there does not seem to be much if any negative impact on growth from the bench press when training with light weights. Thus, shorter rest periods for light-load upper body work are a viable option to cut down on training time without sacrificing gains.
* Since single joint exercise does not elicit comparable fatigue to multi-joint movements, it is conceivable that short rest would be similarly viable for single-joint lower body exercises such as the leg extension. This remains speculative, however, as the topic wasn’t directly investigated in our study.
Dating back to my early years as a personal trainer in the mid-90’s, I began to become intrigued by the concept of “loading zones” whereby different rep ranges purportedly could bring about differential effects on muscular adaptations. Prevailing wisdom at the time was that heavy loads (1-5 RM) promote maximal strength gains, moderate loads (6-12 RM) elicit maximal increases in muscle mass, and light loads (15+ RM) produce the greatest improvements in local muscular endurance. This concept, discussed extensively in exercise science texts, was termed the “strength-endurance continuum” (see the image below) although direct research on the topic was limited.
The topic of rep ranges was so intriguing to me that I ultimately made it a focus of my doctoral work. Several years ago I published the data collected in accordance with my dissertation study. In brief, the study looked at muscular adaptations in a “bodybuilding-type” routine versus a “powerlifting-type” routine in resistance-trained men when the routines were equated for volume load. Consistent with the “strength-endurance continuum” concept, the study found that the powerlifting-type routine produced the greatest strength increases. Contrary to prevailing wisdom, however, both routines produced similar increases in hypertrophy of the biceps brachii. You can read my write-up of the routine in this blog post.
Importantly, the findings of that study are specific to the respective routines being equated for volume load. While this provides interesting insights on the topic, it is impractical to carry out long-term training with very heavy loads at the volumes used in that study (in fact, the majority of subjects in the powerlifting-type group displayed clear signs of overtraining by study’s end). So the question arises as to whether results would differ if an equal number of sets were performed between heavy and moderate loads?
What We Did
Nineteen college-aged men were recruited to participate in the study. All subjects had at least one year of resistance training experience lifting at least three times per week. Subjects were randomized to either a group that trained in a heavy loading range of 2-4 repetitions per set (HEAVY) or a group that trained in a moderate loading range of 8-12 repetitions per set (MODERATE). All other aspects of the subjects’ program were kept constant between groups. The training protocol consisted of seven exercises that worked all the major muscles of the body each session, with three sets performed per exercise. Training was carried out on three non-consecutive days per week for eight weeks. Subjects were instructed to maintain their normal daily nutritional intake and no differences in either calories or macronutrient consumption was found between groups over the course of the study.
What We Measured
We tested hypertrophy of the elbow flexors, elbow extensors, and quads using b-mode ultrasound. Maximal strength was assessed in the squat and bench press via 1 repetition maximum (RM) testing. Upper body local muscular endurance was determined by assessing the subject’s initial 1RM in the bench press for as many repetitions as possible to muscular failure.
What We Found
The infographic to the left (courtesy of Thomas Coughlin) illustrates the results of the study. In general, overall muscle growth was greater for MODERATE compared to HEAVY. Increases in thickness of the elbow flexors (i.e. biceps brachii and brachialis) modestly favored the use of moderate reps (~5% vs ~3% for MODERATE vs HEAVY, respectively) while gains in the quads substantially favored the moderate rep group (10% vs 4% for MODERATE vs HEAVY, respectively). Interestingly, growth of the triceps was similar between groups.
On the other hand, strength gains were decidedly greater when training with heavy loads. This was seen for improvements in both the 1RM squat (29% versus 16%) and bench press (14% vs 10%), which favored HEAVY compared to MODERATE. Muscle endurance increases were similar between rep ranges.
What are the Practical Implications
The study provides evidence that training with heavy loads helps to maximize muscle strength and training with moderate loads promotes greater increases in muscle mass. Importantly, these findings are specific to routines where the number of sets are equated. At face value, this is consistent with the “strength-endurance continuum” and supports what gym bro’s have been preaching for years in regards to rep ranges.
However, when the results are taken into account with my previous study on the topic that equated volume load, an interesting hypothesis emerges. Since strength gains were greater with heavy loads in both studies, it can be concluded that low-rep training is best for maximizing strength regardless of volume load. On the other hand, since the previous study showed no differences in hypertrophy between conditions when volume load was equated, it can be inferred that volume load is a greater driver of muscle growth irrespective of the rep range. In other words, strength is maximized even with lower training volumes provided heavy loads are used, but higher volumes are needed to maximize gains in size whether you train with moderate or heavy weights.
The study had several limitations including a relatively small sample size, the use of a single-site measurement for muscle growth on each of the respective muscles, and possible confounding from the “novelty factor” (i.e. virtually all the subjects trained with moderate loads, so it is possible that the novel stimulus for those in the heavy load group might have impacted results). These issues must be taken into account when attempting to draw evidence-based conclusions. Most importantly, one study is never the be-all-end-all when it comes to answering questions on an applied science topic. Rather, each study should be considered a piece in a puzzle that lends support to a given theory. The practical implications of programming loading zones will become increasingly clear as we continue to build on this line of research. For now, though, the evidence suggests to train heavy if your goal is maximal strength, and to focus on accumulating volume for maximal gains in muscle mass.
The question as to how much strength training volume is needed to maximize muscular gains has been an ongoing source of debate, both in scientific circles as well as the realm of social media. Some claim that a very low volume approach is all that’s required while others subscribe to the belief that marathon training sessions are an absolute necessity.
Who’s right? Well…
Back in 2010, my colleague James Krieger carried out a meta-analysis to provide evidence-based clarity on the topic. In case you’re not aware, a meta-analysis pools data from all relevant studies on a given subject to provide greater statistical power and thus enhance the ability to draw practical inferences from the literature. In short, the analysis showed that performance of multiple sets was associated with a 40% greater hypertrophy-related effect size (a statistical measure of the meaningfulness of results) compared to single-set training.
While this paper provided good evidence in support of higher training volumes, there were some issues with the analysis. For one, James only looked at sets per muscle per workout; a potentially more important marker in determining the hypertrophic response is the weekly volume per muscle group. Moreover, only 8 studies qualified for inclusion in James’ analysis at the time, and only 3 of these studies used direct site-specific measures of muscle growth (i.e. MRI, ultrasound, etc).
Since publication of James’ meta-analysis, a number of additional studies have been published in the peer-reviewed literature. Given this info and in an attempt to resolve previous issues, James and I decided it was appropriate to carry out a follow-up meta-analysis that encompassed all the evidence to date. We recruited our colleague Dan Ogborn to collaborate on the project, and centered our focus on the effects of weekly sets per muscle group on changes in muscle mass. I’m happy to report the paper was recently published in the Journal of Sport Sciences.
Here’s the lowdown:
What We Did
A literature search was conducted to locate all studies that directly compared measures of hypertrophy between higher versus lower resistance training volumes with all other variables equated between conditions. Only human studies with healthy subjects that had a minimum duration of six weeks were considered for inclusion.
What We Found
A total of 15 studies were identified that met inclusion criteria. We ran multiple comparisons to assess the topic from different perspectives. First we evaluated the effects of volume within each study and found that higher volumes were associated with a 3.9% greater average increase compared to lower volumes; the findings were statistically significant (i.e. high probability that they weren’t due to chance alone). As shown in the accompanying forest plot, only 1 of the 15 studies showed a favorable effect for lower volume training, emphasizing the high probability that greater volumes produce greater increases in muscle growth.
We next looked at the effects of volume on a two-level categorical basis, splitting the data into performing less than 9 sets versus 9 sets or more. In this model, the lower volume condition was associated with a gain of 5.8% while the higher volume condition produced a gain of 8.2%. Although the results did not reach statistical significance in this model, the probability of an effect was nevertheless very high (p = 0.076).
Finally, we employed a three-level categorical analysis whereby volume was stratified into less than 5 weekly sets per muscle, 5 to 9 weekly sets per muscle, and 10+ sets per muscle. Here we found a graded dose response whereby gains in muscle progressively increased across each category from 5.4% to 6.6% to 9.8%, respectively. As with the two-level model, results did not quite reach significance, but a high level of confidence can be inferred that results were not due to chance alone (p = 0.074).
What are the Practical Implications
There are several important take-aways from our meta-analysis. First off, a low volume approach can build appreciable muscle. Performing less than 5 weekly sets per muscle produced an average hypertrophic gain of 5.4%. Not too shabby. So if you are time-pressed and not concerned about achieving the upper limits of your muscular potential, it should be heartening to know that you can build an impressive physique without spending a lot of time in the gym.
That said, there is a clear dose-response relationship between volume and hypertrophy. In the three way categorical model, performing 10+ sets produced almost twice the gains as performing less than 5 weekly sets per muscle (9.8% vs 5.4%). Performing 10+ weekly sets per muscle was also associated with a markedly greater increase in muscle mass compared to 5-9 sets (9.8% vs 6.6%). Thus, a higher volume approach is clearly necessary if you want to maximize muscular gains.
So how many sets should you perform to maximize hypertrophy? That remains to be determined. While 10+ weekly sets per muscle was established as a minimum threshold, we were not able to determine an upper threshold where optimal muscle growth is achieved. The effects of volume on hypertrophy undoubtedly follows an inverted-U curve, whereby results progressively increase up to a certain point, then level off, and then ultimately decrease at exceedingly high volumes due to the negative consequences of overtraining. Moreover, the adaptive response to volume will be specific to the individual, with some lifters able to benefit from higher volumes more so than others. Thus, experimentation is needed to tweak the number of sets you perform based on how you respond.
It may well be that periodized approach is best here. Given that repeatedly training with high volumes can lead to an overtrained state, cycling from lower to higher volume blocks that culminate in a brief period of functional overreaching would hypothetically allow for sustained muscular gains over time while staving off the potential for overtraining. It’s a strategy that I’ve employed with good success when working with clients.
Interestingly, a previous study indicated that higher volumes were beneficial for the lower but not upper body musculature. A follow-up study by the same research group similarly found that satellite cell activation was dependent on volume only in the lower body musculature. However, our pooled analysis did not support these findings. Rather, volume was equally important irrespective of body region, with higher volumes translating into greater increases in size.
A limitation of the analysis is that the findings are largely specific to the muscles of the upper arms and frontal thighs; there simply isn’t enough evidence to generalize results to other body regions (i.e. muscles of the back, shoulders, chest, calves, etc). What’s more, the vast majority of studies were carried out in untrained subjects; only two studies used resistance-trained individuals. It has been speculated that increasingly higher volumes are necessary as one gains lifting experience, but more research is needed to support such a conclusion. My lab currently has a large scale study in development to investigate the topic in well-trained men that should help to fill in the gaps in the current literature. Stay tuned…
A long-held belief in bodybuilding circles is that your body can only absorb a fairly small amount of protein in a single feeding. The exact dosage varies depending on who you listen to, but it’s generally purported to be somewhere around 20-30 grams of protein per meal.
While the claim is often taken as gospel, let’s take a close look at the research to draw evidence-based conclusions on the topic.
First and foremost, it’s important to note that from a nutritional standpoint the term “absorption” refers to the passage of nutrients from the gut into circulation – and in this context, there is virtually no limit to protein absorption. Once digested, the constituent amino acids of a given protein are transported through the intestinal cells (enterocytes) and then enter the bloodstream – pretty much all the amino acids consumed become available for use by tissues. The only potential issue with absorption is when you ingest individual free-form amino acids, as this can cause competition at the enterocytes whereby the amino acids present in the highest concentrations are absorbed at the expense of those that are less concentrated (6).
The more relevant question here is whether there’s in an upper limit to how much protein your body can use for muscle-building purposes. This question is a lot more complex and an evidence-based answer requires a good deal of extrapolation based on the limitations of current research.
Some researchers have proposed that muscle protein synthesis tops out at approximately 20-25 grams of protein per serving for young adults. Protein consumed above this dosage is thought to be oxidized for energy rather than used for tissue-building purposes – a phenomenon called the “muscle-full” effect (11). In what is often cited as the definitive support for this contention, Areta et al (1) investigated the effect of different protein boluses on resistance-trained men. All subjects performed a bout of resistance training and were then confined to rest where they consumed 80 grams of protein over a 12 hour recovery period in one of the following three conditions: 8 servings of 10 grams every 1.5 hours; 4 servings of 20 grams every 3 hours; or 2 servings of 40 grams every 6 hours. Over the course of the recovery period, the greatest effect on stimulation of muscle protein synthesis was seen in the group consuming 4 servings of 20 grams of protein. This would seem to indicate that there was no added benefit to consuming the higher dosage (40 grams), and that the additional amino acids were indeed oxidized for energy.
Case closed, right?
Not so fast.
Several variables influence the metabolism of protein and amino acids including the composition of the given protein source, the composition of the meal, and the dose of the protein or amino acids consumed (4). Individual factors such as age, training status, and the amount of lean body mass also come into play. The subjects in the Areta et al study consumed only whey protein during the post-workout period. Whey is a fast-acting protein, with an absorption rate estimated to be up to 10 grams an hour (4). A 20 gram whey bolus therefore would be completely absorbed in a two hour period. Although this rapid assimilation can transiently spike rates of muscle protein synthesis, it also causes a greater oxidation of the constituent amino acids and thus can result in a lower net protein accretion compared to a slow-absorbing protein source (5). On the other hand, cooked egg protein is absorbed at a rate of approximately 3 grams an hour (4). Thus, the same 20 gram protein bolus consumed as an omelet would take over 7 hours for full absorption, potentially allowing for a greater per-meal dosage without causing undue amino acid oxidation. Moreover, in real life you’ll generally be consuming whole foods that contain a combination of carbs and fats along with the protein component. This substantially slows down digestion, resulting in a much more time-released effect on amino acids into the body. In addition, the study only provided only 80 grams of protein over the course of the day to a group of resistance-trained men. This amounts to less than ½ gram per pound of body mass – well below the amount needed to maximize post-workout muscle protein synthesis (9).
A recent study by Kim et al (7) provides contrary evidence on the topic. Subjects came to the lab on two separate occasions: during one session they consumed 40 grams of beef protein and in the other session they consumed 70 grams of the same protein source. One group consumed the protein after a total-body resistance training bout while another did so in the absence of exercise. Results showed that while both conditions promoted increases in whole body nitrogen balance – a marker of anabolism – the higher protein intake resulted in a significantly greater anabolic response, which was largely attributed to a greater reduction in protein breakdown. A major difference between this study and that of Areta et al (1) is that subjects consumed mixed meals containing not only protein, but carbohydrates and dietary fats as well. Thus, the transit time of protein release would necessarily be much slower in this study, potentially accounting for dose-dependent differences in anabolism.
A limitation of the Kim et al study is that measures of anabolism were not specific to muscle but rather taken at the whole-body level. It is likely that much of the superior anabolic response noted with the higher protein intake was from tissues other than muscle, most notably the gut. However, protein turnover in the gut can allow these additional amino acids to be released into the bloodstream and subsequently used for muscle protein synthesis. The extent to which this phenomenon affects muscle-building is not clear, but it conceivably provides the potential for enhanced muscular gains.
While the results of the aforementioned studies provide a sound basis for speculation, it is important to note that measures of acute muscle protein synthesis do not necessarily correlate with muscular gains achieved from consistent lifting (10). To get a true grasp on the upper limit to protein intake in a single sitting, we need to look at long-term training studies that measure actual changes in lean mass.
Several studies have endeavored to investigate the effects of per-meal protein dosage on body composition over time. Arnal et al (2) found that feeding elderly women the bulk of their daily protein (79%) in a single meal (skewed condition) promoted greater retention of lean body mass versus spreading out consumption evenly over four daily meals (spread condition). A follow-up study by the same lab found no differences between skewed and spread protein feedings in a cohort of young women (3). The combined findings suggest that at the very least, consuming the majority of daily protein as a large bolus is not detrimental to lean mass accretion. Unfortunately, total protein intake in these studies was on the low side (~1 g/kg/day), and none employed a resistance training program. Thus, it is difficult to generalize findings to resistance-trained individuals seeking to maximize muscle mass.
Studies on intermittent fasting shed additional light on the topic. These protocols generally involve consumption of nutrients in a very limited time-frame – usually less than 8 hours – followed by a prolonged fast. A recent systematic review found that the majority of intermittent fasting protocols had similar effects on lean body mass compared to traditional eating patterns (12). But again, the studies involve suboptimal protein intakes without a resistance training component – and here the subjects were all in a caloric deficit. Not very applicable to the hard-training lifter.
Considering the limitations of the body of literature, here’s the take-home message based on current evidence: While certainly a threshold exists beyond which protein will be oxidized for energy rather than used for tissue-building purposes, the amount appears to be well above the often cited 20-30 gram limit provided that nutrients are obtained from whole-food based mixed meals. Given that the anabolic effect of a protein-rich meal lasts approximately 5-6 hours (8), a good rule-of-thumb for maximizing muscle growth would is to consume a minimum of 3-4 evenly distributed daily meals containing at least 30 grams of a high quality protein. Within these boundaries, it probably doesn’t matter how you allocate the rest of your protein consumption on a per-meal basis – just make sure you take in close to a gram per pound of body weight per day.
1. Areta, JL, Burke, LM, Ross, ML, Camera, DM, West, DW, Broad, EM, Jeacocke, NA, Moore, DR, Stellingwerff, T, Phillips, SM, Hawley, JA, and Coffey, VG. Timing and distribution of protein ingestion during prolonged recovery from resistance exercise alters myofibrillar protein synthesis. J. Physiol. 591: 2319-2331, 2013.
2. Arnal, MA, Mosoni, L, Boirie, Y, Houlier, ML, Morin, L, Verdier, E, Ritz, P, Antoine, JM, Prugnaud, J, Beaufrere, B, and Mirand, PP. Protein pulse feeding improves protein retention in elderly women. Am. J. Clin. Nutr. 69: 1202-1208, 1999.
3. Arnal, MA, Mosoni, L, Boirie, Y, Houlier, ML, Morin, L, Verdier, E, Ritz, P, Antoine, JM, Prugnaud, J, Beaufrere, B, and Mirand, PP. Protein feeding pattern does not affect protein retention in young women. J. Nutr. 130: 1700-1704, 2000.
4. Bilsborough, S, and Mann, N. A review of issues of dietary protein intake in humans. Int. J. Sport Nutr. Exerc. Metab. 16: 129-152, 2006.
5. Dangin, M, Boirie, Y, Guillet, C, and Beaufrere, B. Influence of the protein digestion rate on protein turnover in young and elderly subjects. J. Nutr. 132: 3228S-33S, 2002.
6. Gropper, SS, Smith, JL, and Groff, JL. Advanced Nutrition and Human Metabolism. Belmont, CA; Wadsworth Cengage Learning, 2009.
7. Kim, IY, Schutzler, S, Schrader, A, Spencer, HJ, Azhar, G, Ferrando, AA, and Wolfe, RR. The anabolic response to a meal containing different amounts of protein is not limited by the maximal stimulation of protein synthesis in healthy young adults. Am. J. Physiol. Endocrinol. Metab. 310: E73-80, 2016.
8. Layman, DK. Protein quantity and quality at levels above the RDA improves adult weight loss. J. Am. Coll. Nutr. 23: 631S-636S, 2004.
9. Lemon, PW, Tarnopolsky, MA, MacDougall, JD, and Atkinson, SA. Protein requirements and muscle mass/strength changes during intensive training in novice bodybuilders. J. Appl. Physiol. 73: 767-775, 1992.
10. Mitchell, CJ, Churchward-Venne, TA, Parise, G, Bellamy, L, Baker, SK, Smith, K, Atherton, PJ, and Phillips, SM. Acute post-exercise myofibrillar protein synthesis is not correlated with resistance training-induced muscle hypertrophy in young men. PLoS One 9: e89431, 2014.
11. Morton, RW, McGlory, C, and Phillips, SM. Nutritional interventions to augment resistance training-induced skeletal muscle hypertrophy. Front. Physiol. 6: 245, 2015.
12. Seimon, RV, Roekenes, JA, Zibellini, J, Zhu, B, Gibson, AA, Hills, AP, Wood, RE, King, NA, Byrne, NM, and Sainsbury, A. Do intermittent diets provide physiological benefits over continuous diets for weight loss? A systematic review of clinical trials. Mol. Cell. Endocrinol. 418 Pt 2: 153-172, 2015.
Wanted to keep you updated on all that is going on at the moment. So much to share!
In case you haven’t heard, my newest consumer book called Strong and Sculpted, was released a few weeks ago. Happy to report it’s been the top-selling new book in Amazon.com’s “weight training” category and has gotten stellar reviews from consumers and pros alike. It’s a scientifically-based handbook for optimizing muscle development, providing step-by-step guidelines for program design. Check it out! In addition, my upcoming textbook called, Science and Development of Muscle Hypertrophy, is scheduled to be released at the end of the month. It will be the first text to provide an evidence-based perspective on muscle growth, covering all the research and its practical implications. If you’d like to be amongst the first to receive the book, it’s now available for pre-order on Amazon.com at a 20% discount.
A recent study published in the Journal of the International Society of Sports Nutrition reported that branched chain amino acid (BCAA) supplementation helped accelerate fat loss while preserving lean mass in trained individuals performing resistance training when dieting. On the surface, this would seem to provide compelling evidence of a benefit to supplementation. However, after scrutinizing the study’s methods, my colleagues Alan Aragon, Brad Dieter, and I found some glaring issues with the statistical procedures and reporting of data. We thus wrote a letter to the edtior detailing these errors and inconsistencies. Give it a read, as it points out the importance of perusing the entire study – not just the abstract – when drawing practical applications from research.
Here’s a vid of my favorite way to perform upright rows. The rope takes stress off the wrists, facilitating movement. Make sure your upper arms don’t go beyond parallel to the ground and your elbows stay above the level of your wrists.
Big shout out to my buddy and partner-in-science Bret Contreras for officially publishing the first long-term study on performance outcomes in the hip thrust versus the squat. Bret has devoted his career to developing a better understanding of how strength and hypertrophy of the hip extensors can be optimized through resistance training, and this study provides an important addition to the literature. I know Bret’s working on a number of follow-ups to further this line of research. Stay tuned.
I have a number of speaking engagements schedule for this summer. First up is Bropocalypse 2016 taking place on June 11th and 12th in Sydney, Australia. I’ll be speaking with uber-colleagues Alan Aragon, Bret Contreras, and James Krieger on what will be a terrific weekend of evidence-based learning. Next up is the NSCA National Conference in New Orleans this July, where I’ll speak on loading strategies for maximizing muscular gains. Then comes the CanFitPro World Expo in Toronto, Canada where I’ll be speaking on a number of fitness- and nutrition-related topics, as well as doing a book sign at the expo. Finally, at the end of August I’ll be in Oslo, Norway at the AFPT Fitness Convention along with some of the best and brightest minds in fitness. Last year’s event was a sell-out so if you’re planning to attend book early!
I recently appeared again on Superhuman Radio to discuss some of my recent research as well as my new book. The host, Carl Lanore, always asks pointed questions that make for a compelling listen.
Last but not least, I’ve uploaded a majority of my recent publications to my ResearchGate page. Included is our recent meta-analysis on training frequency, an original study comparing a daily undulating periodized routine to a traditional hypertrophy protocol, and a study on the effects of conjugated linoleic acid (CLA) on fat loss, amongst others. The PDFs are free to download and soak up the knowledge!
Training frequency is one of the most hotly debated topics in the field of resistance training. While traditionally the term frequency has been associated with how many days a week you work out, a potentially more important variable is the number of times a given muscle group is trained per week.
The internet is littered with varying opinions as to optimal training frequency for maximizing muscle hypertrophy. Some preach the typical bodybuilding “bro-split” which involves training each muscle group once a week with high volumes per session, whereas others propose training each muscle as many as 6 days a week with lower per-session volumes is the best way to get jacked. Problem is, all these opinions are largely anecdotal with limited scientific support. Seems hard to believe, but there hasn’t been a whole lot of research on the topic, and the studies that have been carried out have employed a variety of methodological designs that makes it difficult to sort out a conclusion at face value.
In an attempt to achieve better clarity on the effects of frequency on muscle growth, I recently collaborated on a meta-analysis with colleagues James Krieger and Dan Ogborn. In case you’re not aware, a meta-analysis pools data from all studies on a given subject to provide greater statistical power and thus enhance the ability to draw practical inferences.
Here’s the lowdown:
What We Did
A literature search was conducted to locate all studies that directly compared measures of hypertrophy for different weekly lifting frequencies using traditional resistance training programs. Only human studies with healthy subjects were considered, and study duration had to last a minimum of four weeks.
A total of 10 studies were identified that met inclusion criteria. 7 of the studies, comprising a total of 200 subjects, investigated muscle group frequency while the other 3 studies assessed training session frequency when the number of weekly times working a muscle group was matched.
What We Found
We first looked at the effects of frequency as a binary predictor. Simply stated, this means that the higher frequency condition in a study was compared to the lower frequency condition, irrespective of how many days a week the muscle group was trained. Thus, a 2 day-a-week vs 1 day-a-week was treated the same as a 3 day-a-week vs 1 day-a-week. In this model, there was a clear benefit for higher frequency training of a muscle group. The effect size – a measure of the meaningfulness of results – was 48% greater for the higher frequency conditions (0.49 vs 0.30, respectively), translating into an average hypertrophy increase of 6.8% versus 3.7% for higher vs lower frequencies, respectively. Moreover, as shown in the accompanying chart, every study on the topic showed a benefit to training with higher frequencies.
Due to an insufficient number of studies looking at training 1, 2, or 3 days per week, we were unable to produce reliable estimates on the hypertrophic effects of specific lifting frequencies. Similarly, with only 3 studies looking at training session frequency when groups were matched for frequency of training per muscle group, data was insufficient to produce reliable estimates for effects on hypertrophy.
What are the Practical Implications
The primary take-away from the meta-analysis is that there appears to be a pretty clear benefit to training muscle groups with higher weekly frequencies. At the very least, the study shows that training a minimum of 2 days a week is needed to maximize muscle growth. Unfortunately there simply aren’t enough studies to make more concrete determinations as to the precise number of times that a muscle should be trained each week for optimal growth. Nevertheless, training a muscle just once a week was shown to promote substantial muscle growth. So the claims made by some that the typical bro-split only works for juiced-up bodybuilders are patently false.
It’s important to realize that research studies are relatively short-term, usually lasting 6 to 12 weeks. Problem is, you can’t necessarily extrapolate that results found would continue over time. This is particularly true of a variable such as frequency, as high training frequencies may ultimately lead to an overtrained state and thus have a negative impact on muscle development. Given such a possibility, it may be prudent to periodize training frequency, varying the number of times a muscle is trained each week in a systematic fashion. It also indicates a potential benefit to instituting regular deload periods, where a week of reduced frequency, volume, and/or intensity is strategically integrated into your program every month or so to facilitate recuperation and regeneration.
Importantly, remember that research reports the average responses, but there are generally large inter-individual differences in results. Some may respond best to higher frequencies while others might do better with lower frequencies. Use research to guide your programming, then experiment to see what works best for you.
I was recently interviewed for an article by Men’s Health Magazine on how to target the lower aspect of the abdomninals. As discussed in the article, there is evidence that you can increase activation of the lower abdominal region by initiating a posterior pelvic tilt during performance of exercises such as the reverse crunch and hanging knee raise. Here is a video depicting proper performance:
Now what isn’t clear is whether the increased activation of the lower abs translates into greater muscle development over time. There is emerging research that muscle growth is correlated to the region of greatest activation, but the evidence is far from conclusive at this point. Taking all things into account, there is a potential benefit to performing targeted lower abdominal exercise for those seeking to maximize development in this region. It probably won’t make much of a meaningful difference for the average gym-goer, but for those who aspire to develop their physique to the utmost (i.e. bodybuilders) it may well provide a tangible benefit.
If you follow my work you’ll undoubtedly know that our lab has carried out a number of studies seeking to determine the effects of training in different repetition ranges on muscle strength and growth. The overall findings from these studies showed similar increases in hypertrophy between both heavy and moderate rep ranges, as well as moderate and high rep ranges.
However, the choice of rep ranges is not necessarily an either-or proposition; you can in fact combine strategies to potentially achieve greater hypertrophic benefits. Daily undulating periodization (DUP) routines are specifically designed for this purpose. However, no study to date had compared a varied rep approach to traditional constant-rep training using site-specific measures of muscle growth.
Until now.
Our study, just published in the International Journal of Sports Medicine, set out to investigate if muscular adaptations would differ between DUP-style routine and a traditional hypertrophy-style protocol. Here’s the scoop.
What We Did
Nineteen young men with over four years average resistance-training experience were randomly assigned to 1 of 2 experimental groups that trained 3 days per week: a constant-rep protocol (CONSTANT) that trained using a standard bodybuilding rep range of 8-12 RM per set, or a DUP-style varied-rep protocol (VARIED) that trained with 2-4 RM per set on Day 1, 8-12 RM per set on Day 2, and 20-30 RM on Day 3. All subjects performed a total-body routine consisting of the following seven exercises per session: flat barbell press, barbell military press, wide grip lat pulldown, seated cable row, barbell back squat, machine leg press, and machine knee extension. We tested subjects for changes in hypertrophy of the arm flexors, elbow flexors and quads, as well as maximal strength in the squat and bench press, and upper body muscle endurance. Training was carried out over an 8-week period, with testing done pre- and post-study.
What We Found
Both groups significantly increased markers of muscle strength, muscle thickness, and local muscular endurance. No statistically significant differences were found between conditions in any of the outcomes studied. Sounds like it really doesn’t matter which option you choose, right?
Well, not so fast…
It’s important to understand that the term “statistically significant” simply refers to the probability of results being due to chance at a predetermined level of 5%. This binary method of determining probability has been widely criticized by those in the know about statistics, who proclaim that practical conclusions cannot be drawn merely on the basis of whether a p-value passes a specific threshold. Rather, probability exists on a continuum, and in this regard the p-values (a measure of probability) in our study favored the VARIED condition in several outcome measures. Moreover, magnitude-based statistics (i.e. effect sizes) indicated a benefit to the VARIED condition for upper body hypertrophy, strength, and muscular endurance; no effect size differences were noted for lower body outcomes.
What are the Practical Implications
The study showed a potential benefit – albeit small – to varying repetitions across a spectrum of ranges for increasing upper body muscle strength and hypertrophy. Whether the differences between the varied versus constant rep approach seen in our study would amount to practically meaningful improvements is specific to the individual. For the average gym-goer it probably wouldn’t be of much consequence; alternatively, to a bodybuilder or competitive athlete it very well may. It’s not clear why these findings did not translate into similar differences in lower body muscular adaptions, but based on our findings either approach would seem to be an equally viable choice for leg training.
It’s important to note that this was a relatively short-term study, lasting a total of 8 weeks. When factoring in missed sessions, this means subjects in VARIED trained in each loading zone for a total of only 7-8 sessions over the course of the study period. If the differences in upper body outcomes favoring VARIED would persist over time – highly speculative but certainly possible – the magnitude of results could widen and thus be potentially meaningful for a wide array of fitness enthusiasts.
Another important point is that volume load was consistently lower across all conditions (pushing exercises, pulling exercises, leg exercises, and total volume of all exercises) in VARIED as compared to CONSTANT. This indicates that training in a varied fashion provides comparable or better results with less volume load than training at a constant 8-12 RM repetition range. It also suggests that if volume load were equated between conditions, there might have been even better results for the varied approach.
In sum, our study shows that both varied and constant loading schemes are viable strategies to increase strength and hypertrophy in resistance-trained men. The data suggest a potential modest benefit to varying loading ranges over time, at least for maximizing upper body muscular adaptations. Importantly, findings clearly indicate that contrary to what many believe, training in the “hypertrophy zone” (6-12 RM) is not superior for building muscle. When considering the practical implications of the findings, remember that exercise prescription is always a function of the needs/abilities/goals of the individual.




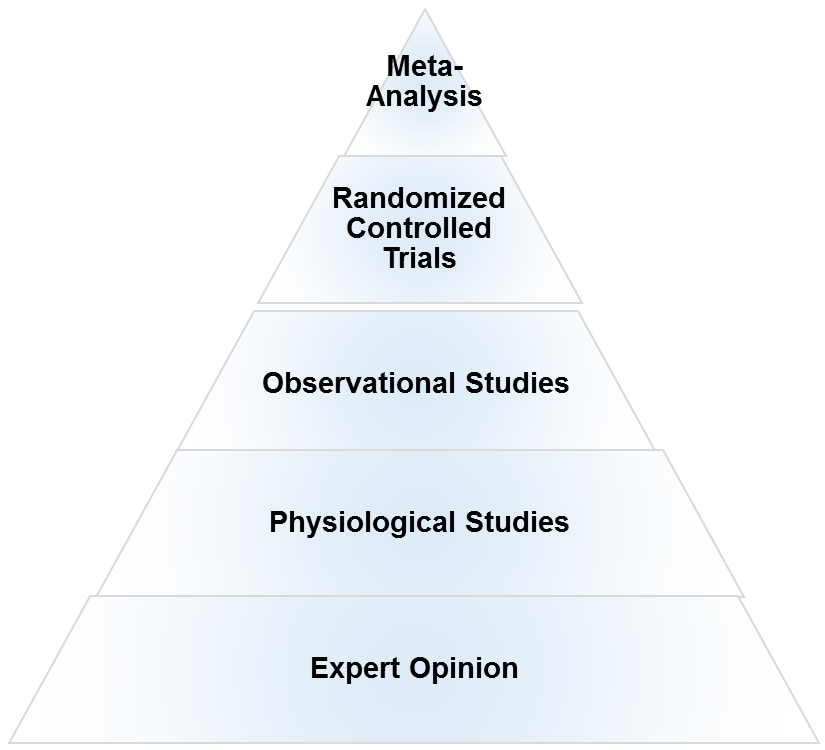

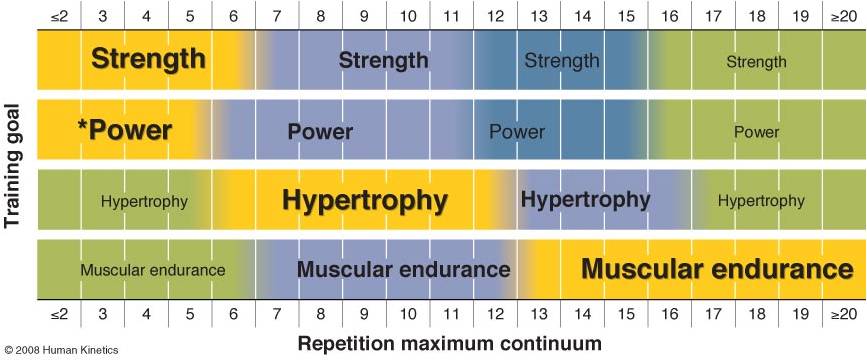
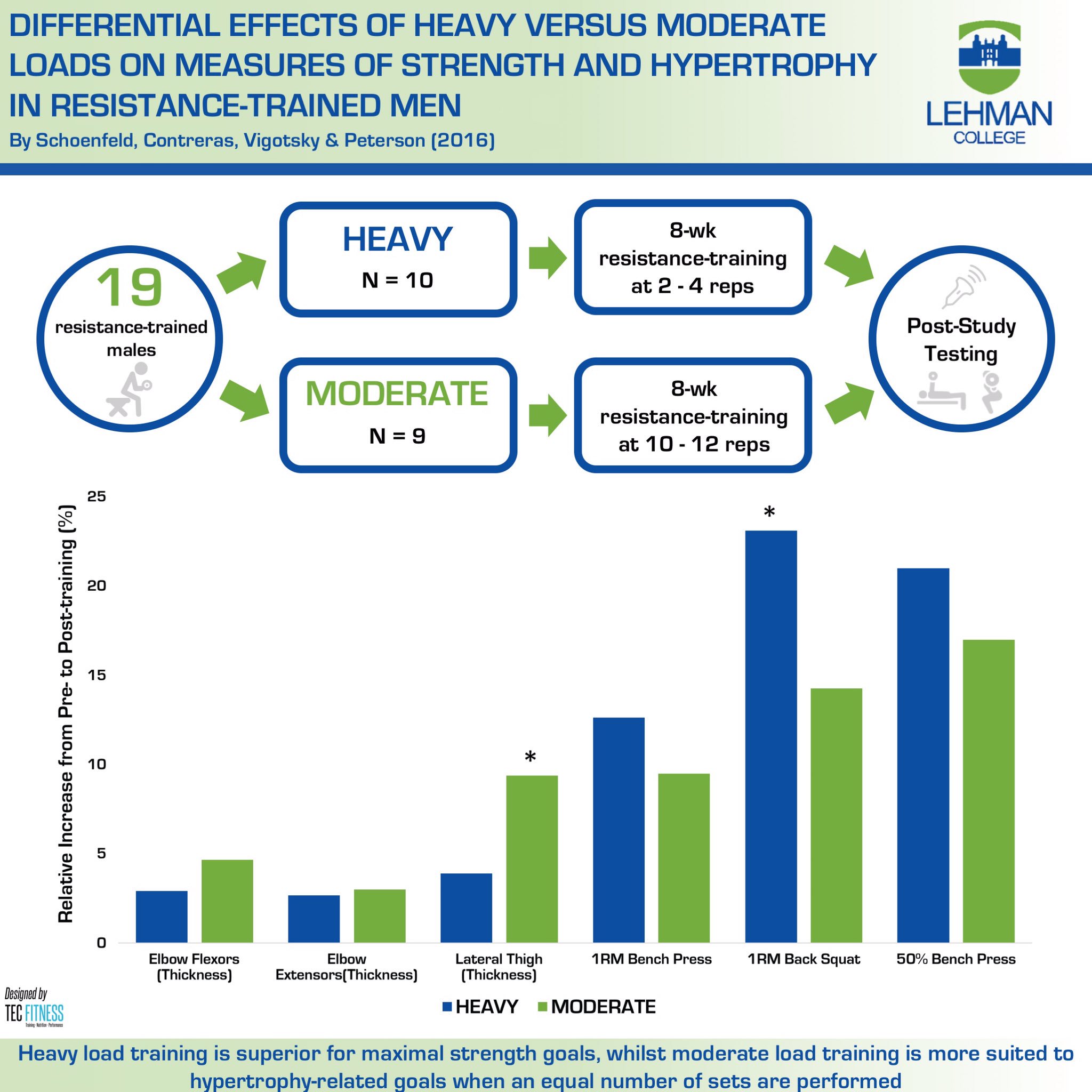
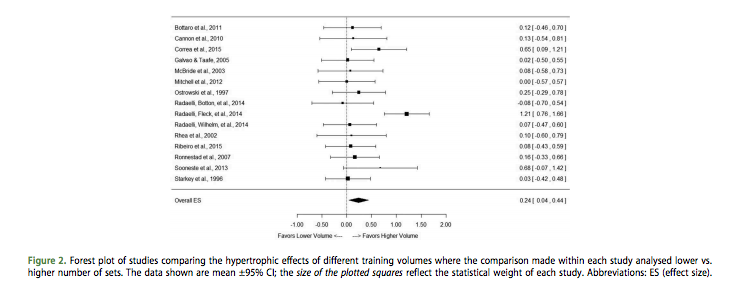
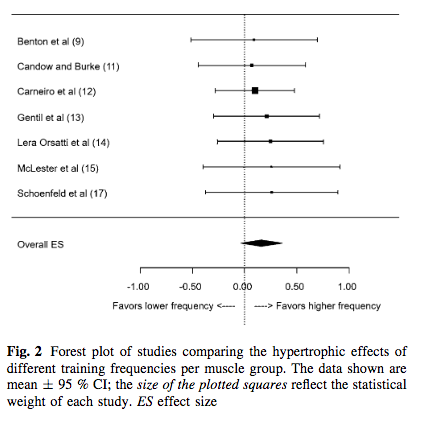
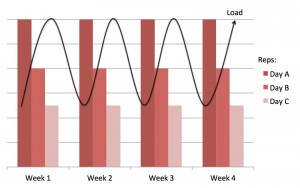
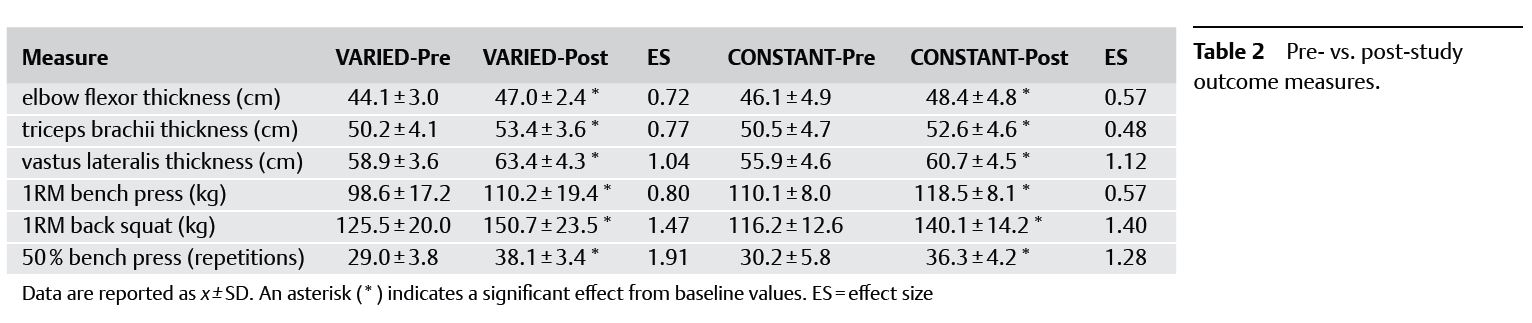
 Entries (RSS)
Entries (RSS)



