Cold water immersion (a.k.a., “ice baths”) has become a popular method amongst exercise enthusiasts and athletes to enhance recovery after an intense training bout. The strategy involves exposing either the trained limb or the whole body to very cold liquid temperatures. According to p...
Brad Schoenfeld, Ph.D, C.S.C.S., is an internationally renowned fitness expert and widely regarded as one of the leading authorities on body composition training (muscle development and fat loss). He is a lifetime drug-free bodybuilder, and has won numerous natural bodybuilding titles.
We are glad that more and more people are demanding and applying evidence in the exercise and nutrition field. That been said, there remains a lot of misunderstanding and misconceptions about an evidence-based Practice (EBP). In this article, we will address some of the common misconceptions and criticisms of EBP. Here we go:
Why do we need EBP? Why can’t we just use anecdotal evidence or expert opinion?
In fact, we’ve used anecdote or expert opinion as ‘evidence’ to treat people throughout the history of medicine. But this approach clearly didn’t work well as shown by hundreds of examples of medical mistakes we made in the past. For example, smoking was ‘good’ for heath until studies showed otherwise; bloodletting was the standard medical treatment for almost 2000 years by the foremost doctors of the West, and so forth. In short, EBP evolved because anecdotal evidence or expert opinion were not producing ‘results’.
The definition of EBM (Evidence Based Medicine) by David Sackett reads: “EBM is a systematic approach to clinical problem-solving that allows integration of the best available research evidence with clinical expertise and patient values”. This principle can be applied across many scientific disciplines, including exercise and nutrition, to optimize results.
What is the evidence?
Many people wrongly assume that the term “best available evidence” in EBM/EBP is limited to research-based evidence. In fact, evidence can be obtained from a well conducted randomized controlled trial, an unsystematic clinical observation, or even expert opinion. For example, the evidence could come from a controlled trial, your favorite fitness guru, or a physiological mechanism. However, the critical point is that the importance or trust we place on the evidence differs based on the type of evidence. We will talk more about this as we talk about the evidence hierarchy.
What about values and preferences?
Every patient or client assigns his/her own values, preferences, and expectations on outcomes and decisions.
For example, some might place a high value on muscle growth, whereas others would value their general health as most important. Some would value building their upper body muscles more than their lower body muscles. Others may value the social aspect of working out at a gym more than the muscle and strength gains.
And rightly so, these personal decisions have no wrong or right and should be listened to and respected. The job of a fitness professional is to help clients achieve whatever goals they desire; we cannot impose our own values no matter how contrasting beliefs and opinions maybe.
What about clinical expertise? And what is the ‘art’ of EBP that people always talk about?
Clinical expertise is what many refer to as the art of EBP. So, does the art of EBP mean applying what has worked for your clients? Clearly not.
Clinical expertise involves basic scientific knowledge, practical expertise, and intuition to:
• diagnose the problem (for example, why can’t this person squat deep, how to correct exercise technique, why he/she is not gaining strength or losing weight.),
• search for the relevant research evidence (how many sets to gain muscle for an advanced trainee, or which exercise targets specific muscles) and critically analyze the research evidence for methodological issues (was the study in beginners, was the outcome measured relevant)
• understand both the benefits, the risks involved, and other alternative approaches to the goal (a Crossfit type workout might be motivating and improve general cardiovascular endurance, but has a high risk of injuries)
• alter the program based on the client feedback and results (reducing the number of sets or modifying the exercise (angles, ROM and do forth) for an older person or someone with pre-existing shoulder injuries.)
• Listen and understand clients value and preferences, clearly communicate the risk, cost, benefits in a simple manner, and use a shared decision approach to come to a decision
And this is called the art of evidence-based approach. As you can see, it forms an integral part of EBP and no amount of research can replace it. Likewise, no amount of clinical expertise can replace research evidence.
What is the evidence hierarchy? And why are RCT’s (Randomized Clinical Trial) at the top of the pyramid?
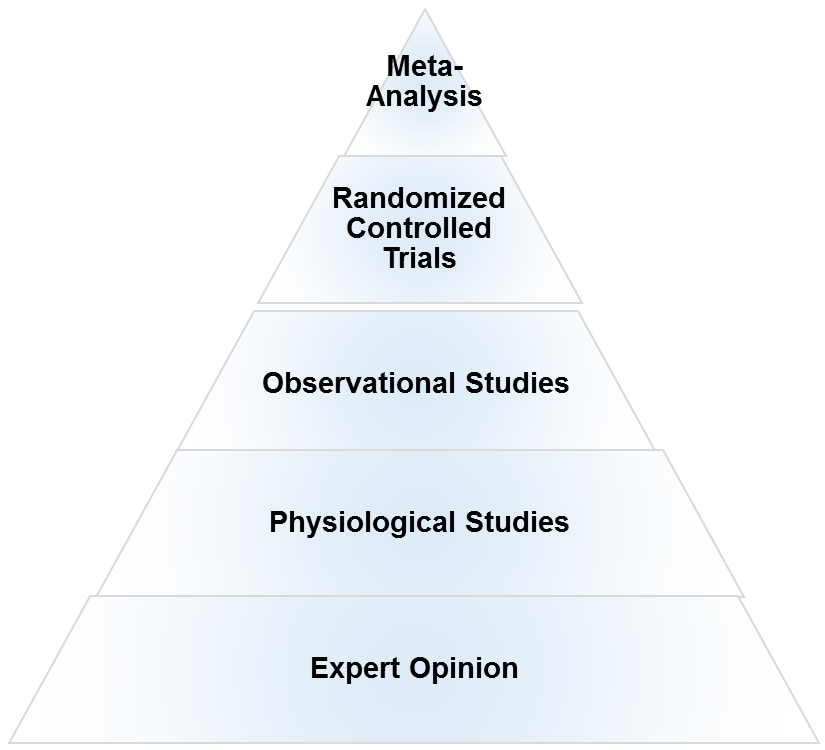
An evidence hierarchy is one of the foundational concepts of EBP. And there are three important points to keep in mind:
• First, as shown, the different types of evidence are arranged in an orderly fashion. As we go up the hierarchy, the trust or the confidence we place in the study results go up too. RCT’s are the most valid research design, as they allow the ability to infer causality. And expert evidence is the least trustworthy and occupies the bottom position. Meta-analyses- a collection or a group of RCT’s-are generally considered the highest form of evidence, as they synthesize the entire body of literature on a given topic and quantify the results based on a statistical measure of practical meaningfulness. Meta-analyses can be particularly important in exercise- and nutrition-related topics, as the sample sizes are often small and thus pooling the data across studies provides greater statistical power for inference.
• Second, it is important to note that depending on the quality of the study, an RCT can be downgraded, too. A poorly designed study will never provide a high level of evidence, and in fact can impair the ability to draw proper evidence-based conclusions. The hierarchy therefore is not set in stone.
• Third, there is always evidence. So the best available evidence is what is available and need not come from an RCT (Randomized Controlled Trial). But based on the type of evidence, our confidence in the results and our recommendations will differ accordingly.
What if there are no RCT’s? How do I evaluate a program or diet?
First, as mentioned before, there is always evidence. If there are no RCT’s, you simply move down the evidence hierarchy. But as you go lower in the hierarchy, uncertainty about the validity of the evidence goes up as well. Second, you also must compare the benefits, risks, cost, scientific plausibility, and other alternative programs before making recommendations. Below are a few examples where the absence of an RCT does not preclude recommendations.
Example 1: If a client comes with a new program that uses 5 lb weights to increase strength, we know from basic science that without load progression, muscle and strength gains will be nil. Such a program would go against the most fundamental theory of muscle growth. So you can make a strong recommendation against the program, even without an RCT.
Example 2: Recently, the Ebola virus vaccine was used before conducting an RCT. How is that possible? Here is a classic example of weighing the benefits, risks, alternative approaches, and making a strong recommendation with weak evidence. In this case the risk is death, the benefit is obvious, and there are no alternative approaches. Thus, the risk/reward strongly favored giving the vaccine. And 99% of the informed patients would agree with the recommendation.
Example 3: If a client wants to try the Xfit program, you can convey the lack of studies (weak evidence), the risks involved, the time required for learning the right technique, and give other programs which are in line with her/his goals. If he/she still wants to do it, he/she shouldn’t be critiqued for their decision.
Example 4: An observational study shows that eating meat raises cancer. Considering observational studies are lower in the hierarchy no matter how well the study is conducted, recommendations cannot be more than just suggestions.
What if there are no studies and my client wants to try a new program?
As previously noted, if a person understands the uncertainty due to the lack of studies or weak evidence, availability of alternative programs that fit his/her goal, the cost, and risks, he/she can make an informed personal choice. Keep in mind that majority of the questions in exercise and nutrition are of weak evidence. In fact, it is the same for the medical field too. But what is important is to clearly know and convey what your recommendations are based on.
There are a lot of factors like genetics, diet, motivation that can influence your results. A study hence…
Many people are unaware that in a randomized controlled trial, the randomization serves a crucial purpose: The randomization ensures, at least theoretically, that both the known variables and unknown variables that can affect muscle growth or strength are equally distributed into both groups. That is, if there are unknown genetical factors that can drive muscle growth, it is highly likely these genetically gifted individuals will be distributed evenly. This is the reason why RCT are considered to be the gold standard to study cause and effect. Hence, the results of the study can be pinned to the intervention or treatment
There are numerous problems with scientific study. So you cannot use the results of a study to train your clients?
Yes. But one of the basic steps in EBP is to critically analyze the study: If the study has methodological issues or has a different population than your client, you downgrade the evidence accordingly and lower your strength of recommendations.
Most of the studies in bodybuilding/strength training are on untrained individuals.
Yes. And rightly so, caution should be used when extrapolating recommandations to trained individuals. Exercise science is a relatively new field and studies in trained individuals are small in number, but accumulating. Generalizability (i.e. the ability to apply findings from a study to a given population) must always be taken into account when using research to guide decision-making.
I don’t care about “why” it works or the science behind. All I care about are results.
As previously mentioned, EBP evolved to get better results. It didn’t evolve to explain how or why a treatment works. There are 1000’s of life saving treatments and drugs where the underlying mechanism(s) are just unknown.
Studies are looking at an average of the sample. There is a lot of individual differences.
Yes. In fact, n=1 studies occupy the top of the evidence hierarchy because it applies to the specific individual in question. But these are hard and almost impossible for certain outcomes like muscle growth or disease prevention. There are two concerns with so-called trial and error method that is often talked about.
• First, even if you gain benefits with a certain program, in many cases, it is extremely hard to figure out what was the variable that made the difference. Was it the specific exercise, the change in diet, the placebo effects, genetics, or some unknown variable?
• Second, it may not be clear if you are indeed making an improvement depending on the outcome. For example, gains in muscle come very slowly for trained individuals (like years for a several pounds). Hence, you will have to run a program for a few years to see if it works or not. However, controlled research often uses measures that are highly sensitive to subtle changes in muscle mass, and thus can detect improvements in a matter of weeks.
The program worked for me!
What was the outcome measure? Strength, muscle growth, weight loss? What are you comparing against? Against your previous results? What was the magnitude of the benefit? Without knowing answers to these questions, the meaning of the word ‘worked’ is unclear.
Further, if it indeed worked, we still don’t know what made it work, or if it will work for someone else. So your personal anecdotes are often fraught with problems and unfortunately mean very little. And importantly, just because something “worked” doesn’t mean that another approach might not work better.
This X supplement was shown to increase muscle growth in an animal study. Should I use it?
Research in animal models is almost at the bottom of the evidence hierarchy. It is very weak and hence the uncertainty is high, and deserves no greater than a weak recommendation. Although animal models can serve an important purpose in preliminary research, evidence based practice should rely primarily on human studies when developing applied guidelines.
A lot of the research is sponsored by nutritional and exercise machine companies. Hence not trustworthy.
Yes. If there is a conflict of interest, the study is downgraded.
I saw a supplement study which showed a statistically significant weight loss. Can I use that supplement for my client?
No, you also have to look at how much weight the subjects lost. The term “significance” is a function of the probability of results occurring by random chance; it is not necessarily related to the magnitude of the effect. Provided a large enough sample size, results of a study can be statistically significant even with just a 1 lb weight loss over a 1 year period. This is known as ‘clinical significance’.
Would you take a supplement to lose 1 lb in a year? Depending on the cost, the burden of taking a pill every day, and how much you value weight loss, you may or may not.
EBP does not consider a science-based approach.
EBP does consider a science-based approach. A science-based approach provides strong evidence when the program or treatment violates fundamental principles or universal laws. For example, homeopathy.
However, EBP does not support evidence just based on biological plausibility or mechanistic evidence. For example, if a new diet tells you to eat as much as you want to lose weight, it goes against fundamental laws of thermodynamics. You do not need an RCT to make strong recommendations against this diet
“This house believes that in the absence of research evidence, an intervention should not be used” This was the motion of a debate which took place at the end of the recent PhysioUK2015 Conference in Liverpool.
As you know by now, EBP does not exclusively rely on RCT’s. To quote the famous saying in EBP: “There is always evidence”. It is an unfortunate misrepresentation of EBP/EBM to assume that without RCT’s, a treatment cannot be recommended. For example, smoking has perhaps the greatest detrimental effect on health of any social habit, and health-based organizations universally recommended against its use. But we do not even have even a single RCT on smoking!
Effects of smoking are from observational studies. But since the magnitude of harm is very high, it upgraded in the evidence pyramid. Once again, this shows why the hierarchy is not set in stone.
‘Parachute use to prevent death and major trauma related to gravitational challenge’. This is the title of the paper published in BMJ. The paper satirically argues that parachute use has not been subjected to rigorous evaluation by using RCTs’ and therefore has not been shown to save lives. Critics of EBP have used this as a criticism of EBP and the reliance of RCT’s.
EBP has always maintained that RCT’s are not required when the magnitude of benefits is very high.
For example, insulin injection for diabetes, Heimlich maneuver, and anesthesia are all examples of treatments where the magnitude of benefit is very high, and hence RCT’s are not required nor asked for.
I do not have enough knowledge to critically analyze studies.
In closing, we hope the article has helped you better appreciate and understand this simple framework called evidence based practice or evidence based medicine. EBP is currently the best approach we have to make decisions related to health, fitness or strength and conditioning. A good EBP practitioner should have a strong understanding of both the practical and the scientific aspects of exercise and nutrition; and more importantly, an untiring commitment and empathy to your clients and their values and preferences.
Proper manipulation of program variables is essential for maximizing the hypertrophic response to resistance training. Variations in volume, loading and rest intervals all have been shown to impact muscular adaptations.
One variable that hasn’t received as much attention is lifting tempo – i.e. how fast you perform a repetition. When you’re using very heavy loads this is moot; although you’ll necessarily need to try to move the weight quickly, the actual concentric speed will be fairly slow. To illustrate this point, a study by Mookerjee and Ratamess found that the first concentric repetition of a 5RM bench press took 1.2 seconds to complete while the fourth and fifth repetitions took 2.5 and 3.3 seconds, respectively. These findings occurred despite subjects being instructed to perform the reps explosively.
When the loads are lightened, however, you have a lot more control over lifting cadence. A wide range of volitional tempos are possible depending on the magnitude of load. Recommendations on the topic are highly disparate depending on who you listen to. Some fitness pros advocate explosive lifts while others recommend slowing tempo down to where a single repetition takes 45 seconds to complete as seen in this video
In an effort to synthesize the evidence and gain clarity on the issue, I collaborated on a meta-analysis with uber-pros James Krieger and Dan Ogborn. The study titled, Effect of repetition duration during resistance training on muscle hypertrophy: a systematic review and meta-analysis was recently published in the journal, Sports Medicine. In case you’re not aware, a meta-analysis pools data from all studies on a given topic and then statistically quantifies the results to provide a gauge of how meaningful the differences are between conditions.
Here’s the scoop.
What We Did
An extensive search of the literature was carried out for randomized controlled trials that directly compared the effects of different training tempos on muscle hypertrophy in healthy individuals. Studies had to last a minimum of 6 weeks and both groups had to perform reps to the point of momentary concentric muscle failure. A total of 8 studies comprising 204 total subjects ultimately met inclusion criteria – a surprisingly low number for such an important topic.
What We Found
There was no difference in hypertrophy between lifting durations of 2 to 6 seconds when using dynamic constant external resistance (typical free weights and machines). A single study using isokinetic dynamometry showed that durations of a half-second up to 8 seconds produced similar hypertrophy, although the generalizability of this study to traditional training methods is somewhat questionable.
There does seem to be a threshold as to how slow you can go, as evidence suggests that “superslow” lifting (i.e. durations above 10 seconds) is suboptimal for hypertrophy. The research on this topic is limited thereby making it difficult to draw firm conclusions, but a recent study found that a traditional speed group increased muscle cross sectional area by 39% compared to only 11% in a group performing reps at a tempo of 10 seconds up, 4 seconds down. These results held true despite an almost five-fold greater time-under-tension for the superslow group. A follow-up study by the same lab showed satellite cell content and myonuclear domain – important components in the ability to increase muscle mass over time – were substantially greater with traditional compared to superslow training. These findings are consistent with research showing that muscle activation is reduced up to 36% when training at very slow speeds (5 seconds concentric and eccentric). And since maximal hypertrophy is predicated on recruiting the full spectrum of muscle fibers and keeping them stimulated for a sufficient period of time, it is logical to speculate that training in a superslow fashion is inferior if your goal is to optimize muscular gains.
What are the Practical Implications
Current research indicates that a wide range of lifting durations can be used to maximize hypertrophy. Given the limited number of studies and their diverse methodology, however, the topic is far from settled. Based on the evidence it would seem prudent to take no more than about 3 seconds on the concentric portion of the movement. Beyond this cadence, you’d need to reduce the load to a point where it could negatively impact the ability to fully stimulate the highest threshold motor units. Eccentric actions should be performed so that the load is controlled against the forces of gravity; simply letting the weight drop fails to provide sufficient muscular tension for the majority of the action (and it also increases the risk of joint-related injury). As with concentric actions, there does not seem to be any advantage to slowing the movement down to more than about 3 seconds and it is possible that doing so might actually be detrimental to growth. I’d add that the reps should be carried out with sufficient control so that a mind-muscle connection can be established with the target musculature – the current body of evidence suggests that such a strategy is beneficial for maximizing muscle activation, which may in turn lead to greater gains.
I’ll note that the above recommendations are rather liberal, giving the benefit of doubt to somewhat slower tempos. My general feeling is that the concentric portion of a rep should be around 1-2 seconds – the most important thing here is to control of the weight by using an internal focus to visualize the target muscle as you lift. Although results of our meta-analysis showed no “statistically significant” differences in tempos up to 3 secs concentric, data from Tanimoto et al show a substantially greater effect size (a measure of the “meaningfulness” of results) for muscle growth favoring traditional (1 sec on concentric and eccentric – effect size 1.08) vs slower (3 secs concentric and eccentric – effect size 0.74) lifting cadences. It therefore would seem a slightly faster tempo is warranted, at least on multi-joint exercises
Could combining different repetition durations potentially enhance the hypertrophic response to training? It’s impossible to say as no study to date has investigated this possibility. As such, the best advice therefore is to experiment for yourself and see if this may spur additional growth. Remember: the best research often comes from what is learned in the trenches!
In a recent interview for The Fitcast, the host asked whether there was anything I’d change about my book The MAX Muscle Plan. A fair question, no doubt. After all, the book was written over four years ago and our understanding of the science and practice of training continues to evolve. So naturally there were several things that I mentioned in retrospect, most pertinently my views on nutrient timing.
But afterward, it occurred to me that I neglected to bring up an important topic of concern; namely, my use of the ratings of perceived exertion (RPE) scale to gauge training intensity of effort. Now don’t get me wrong; the RPE is a viable tool in this regard. Research shows that It provides a reasonably accurate means to predict 1-RM from submaximal lifting intensities. Fitness professionals have used it extensively for years.
That said, previous research found a mismatch between RPE and max effort during sets to failure. A subsequent study showed similar discrepancies.
The literature backs up my personal experience on the topic. Since publication of my book, I’ve received a number of emails from readers saying they were confused about the use of the scale. Some stated they found it awkward to integrate into practice. Others felt that terms such as ‘moderate’ ‘hard’ and ‘extremely hard’ were too ambiguous with respect to exercise intensity of effort.
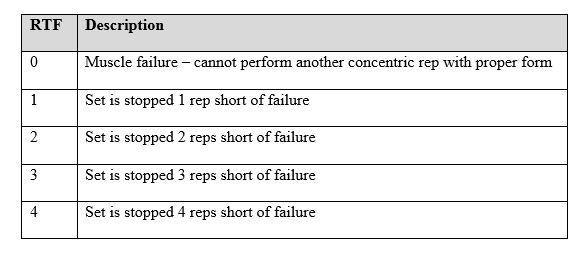
Fortunately, I’ve since come to learn that a more intuitive scale called Reps-to-Failure (RTF) exists. As the name implies, the RTF is based on how many reps you perceive you have left in the tank after completing a set. If you went to all-out failure, the value would be ‘O’ (no reps left in the tank). If you feel you could have gotten an additional rep, the value would be 1; if you could have gotten 2 additional reps you’d be at a ‘2’, etc. I limit the range from 0-4; anything above a 4 is basically a warm-up set. Below is a chart that outlines the particulars of the scale.
The RTF scale has been validated by research. A recent study of competitive male bodybuilders showed a high positive association between estimated RTF and the actual number of repetitions-to-failure achieved. Accuracy was found to improve during the later sets of exercise performance, indicating a rapid learning curve the more the scale is used.
So my recommendation here is to use the RTF scale for gauging lifting intensity; IMO, it’s easier to employ and more accurate than the RPE. If you’re currently using The MAX Muscle Plan simply substitute the RTF value for the RPE in reverse order. Thus, an RTF of ‘0’ corresponds to an RPE of ’10’; an RTF of ‘1’ corresponds to an RPE of ‘9’, etc. It shouldn’t take you more than a few sessions experimenting with the RTF to be thoroughly proficient in its use.
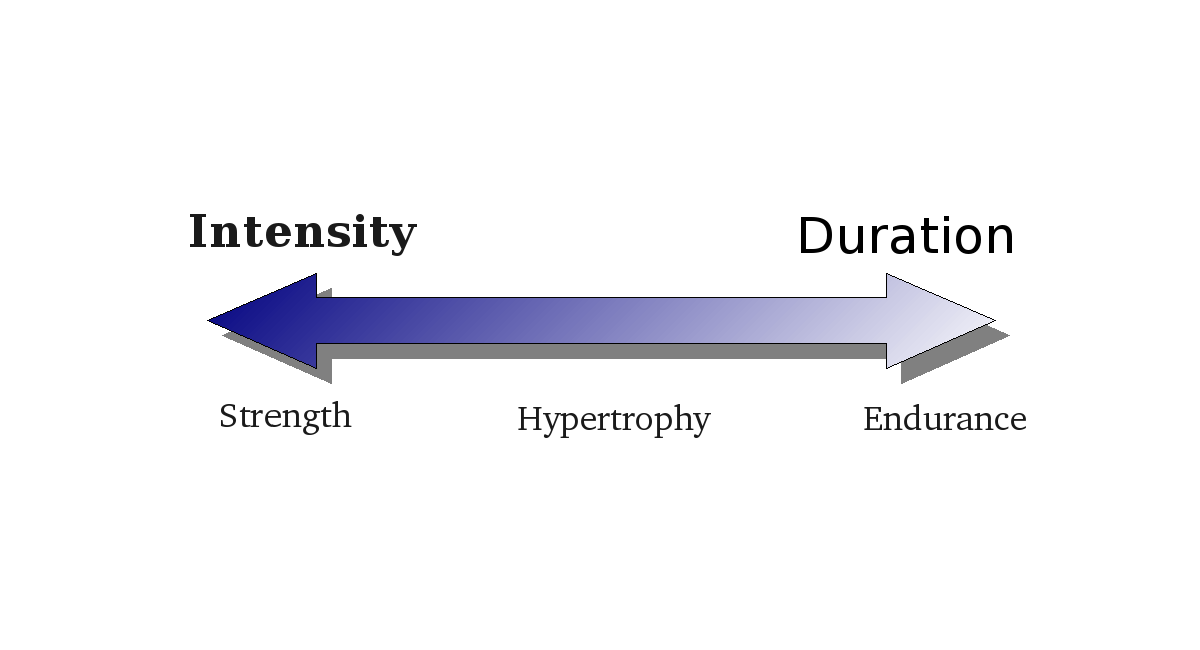
It’s a commonly accepted tenet that resistance training adaptations follow a “strength-endurance continuum” whereby lifting heavy loads maximizes strength increases while light load training leads to optimal improvements in local muscle endurance. Conventional wisdom also postulates that at least moderately heavy loads are required for building muscle. General training guidelines proclaim that loads lighter than about 65% 1RM are insufficient to stimulate fast-twitch muscle fibers necessary for growth. The so-called “hypertrophy range” is generally considered to be 6-12 reps/set.
Recent research has challenged these established tenets. It has been proposed that if light loads are lifted to muscular failure, near-maximal recruitment of fast-twitch fibers will occur resulting in muscular adaptations similar to those obtained from training heavy.
A meta-analysis from my lab published last year in the European Journal of Sports Science found substantial increases in muscle strength and hypertrophy following low-load training. However, the magnitude of increases were not as great as that associated with using heavier loads, and a trend for superior gains was in fact shown when lifting weights >65% 1RM. I covered the specifics of this meta-analysis in a previous post.
The caveat: All previous studies employed untrained subjects, raising the possibility that results were attributed to the “newbie effect” that states those new to training build muscle from pretty much any activity — even cardio!
To achieve clarity on the topic, my lab carried out a well-controlled study on the effects of high- versus low-load training using resistance-trained individuals, which was just published in the Journal of Strength and Conditioning Research. Here’s what you need to know.
What We Did
Eighteen young men with an average of more than 3 years lifting experience were randomly assigned to a resistance training program using either moderately heavy loads (8-12RM) or light loads (25-35RM). All other aspects of the program were held constant between groups to isolate the effects of load on muscular adaptations. The program consisted of 3 sets of 7 different exercises targeting the major muscle groups (bench press, shoulder press, lat pulldown, seated pulley row, back squat, leg press, and leg extension). Training was carried out on 3 non-consecutive days-per-week (M, W, F) for 8 weeks.
Testing was conducted pre- and post-study. We used b-mode ultrasound to measure the thickness of the biceps, triceps, and quads. We assessed maximal strength via 1RM for the back squat and bench press. Finally, we measured changes in muscle endurance by having subjects perform the bench press at 50% of their 1RM to volitional failure.
What We Found
Both groups significantly increased lean mass in their biceps, triceps, and quads, but no statistically significant between-group differences were noted in any of these muscles (i.e. both groups had similar muscle growth over the course of the study). On the other hand, the heavy load group showed significantly greater strength increases in the back squat and a trend for greater increases in the bench press compared to the light load condition. Conversely, local muscle endurance was markedly greater for the low-load group.
Reconciling the Data
The primary take-home points from the study are as follows:
• Gains in muscle mass are about the same regardless of repetition range provided training is carried out to muscle failure
• Maximal strength requires the use of heavy loading
• Muscle endurance is best obtained from the use of light loads
To really understand the practical implications of the study, however, we need to look a bit deeper at the results.
The superior strength gains for heavy load training are consistent with the principle of specificity, which effectively states that training adaptations are specific to the imposed demands. No surprise here. From a mechanistic standpoint, the ability to exert maximal force has a high neural component, and the associated neural adaptations appear to be optimized through the use of heavy loads. Previous work from my lab showed that these adaptations exist even at the far left aspect of the strength-endurance continuum, as a powerlifting-type routine (3RM) was found to produce greater strength increases compared to a bodybuilding-style workout (10RM). It also makes intuitive sense that you need to train heavy to “get a feel” for using the maximal loads required to perform a 1RM.
The greater improvements seen in local muscle endurance from light-load training were expected as well. Although the topic hasn’t been well-studied, it stands to reason that low-load training is associated with adaptations specific to enhancing buffering capacity, thereby allowing for the performance of a greater number of submaximal repetitions. Again, a basic application of the principle of specifity.
On the other hand, I readily admit to being surprised by the fact that muscle growth was similar between conditions. While a number of previous studies had shown no differences in gains between light- and heavy-load training, I figured this was due to the “newbie effect.” No way could you build appreciable muscle using 30 reps per set.
Or so I thought.
I’m now a believer.
What’s particularly interesting, though, are the potential implications for how muscle growth actually manifests when training in different loading zones. A previous study from my lab showed that muscle activation was markedly greater when performing reps at 75% 1RM versus 30% 1RM. A follow up study (currently in review) found that the heavy-load superiority for activation held true when training at 80% 1RM versus 50% 1RM as well. Combined, these findings suggest that the recruitment and/or firing frequency in the high-threshold motor units associated with the largest type II fibers is suboptimal when training at low-loads. It therefore can be hypothesized that if muscle growth is indeed similar across loading zones — as found in the current study — hypertrophy from light-load training necessarily must be greater in the type I fibers. Indeed, emerging research out of Russia indicates that this is in fact that case with multiple studies showing that light loads promote greater gains in type I fibers while heavy loads increase type II fiber hypertrophy to a greater extent (Netreva et al 2007; Netreba et al 2009; Netreba et al 2013; Vinogradova et al 2013).
Bottom line: If your goal is to build as much muscle as possible, it seems appropriate to train across the spectrum of loading zones; use lighter loads to target type I fibers and heavier loads to target type IIs. In this way, you ensure maximal development of all fiber types.
An interesting point to keep in mind is that none of the subjects in my study trained with more than 15 reps/set during the course of their usual lifting routines and the majority never went above 10 reps. This raises the possibility that their endurance-oriented type I fibers were underdeveloped in relation to the strength-oriented type II fibers. If so, it’s possible that their type I fibers had a greater capacity for growth, which was realized in those who trained using light loads.
The study had some notable limitations. For one, the training period lasted only 8 weeks; whether results would have diverged over a longer time-frame is undetermined. For another, muscle thickness was measured only at the approximate mid-point of each muscle. Research has shown that muscles often hypertrophy in a non-uniform manner. Thus, it is possible that other aspects (i.e. distal or proximal) of the muscles studied might have differed in their growth response.
A final and important point to consider. While people often dismiss light-loads as being for wimps, nothing could be further from truth. Training to failure with high reps is highly demanding and the associated acidosis extremely uncomfortable. To this end, approximately half the subjects in the low-load group puked during the first week of training and several others experienced nausea and/or light-headedness. Although these issues tended to dissipate as time went by, they nevertheless can negatively affect adherence to the program. If you choose to incorporate light-loads into your program, be prepared for a grueling workout!
Wanted to update everyone on all that’s been happening; so much to share!
First, I’ve agreed to write a textbook on muscle hypertrophy, to be published by Human Kinetics — one of the leading publishers on the science of exercise and nutrition. The book will be geared towards fitness professionals and university programs. I’m totally stoked to provide an evidence-based resource on a subject that has long relied on gym lore and bro-science. Estimated pub date is April of 2016.
I’ve also agreed to write a monthly column for Flex Magazine. The column will discuss science-based application of hypertrophy and fat loss practices. It’s a real kick for me to be a regular columnist for a mag that I grew up reading. My first column is slated for the November issue.
Research-wise, I’m currently finishing up a study on body comp changes associated with fasted cardio and another on muscle activation during different loading intensities in the bench press. During the fall I have multiple studies set to get underway including a training frequency study investigating muscular adaptations in split vs. total body routines, another comparing functional transfer between the squat and leg press, and yet another that will evaluate the effects of protein timing pre- versus post-workout on muscle hypertrophy in well-trained subjects. I look forward to sharing the results of these and other studies currently in review when they become available.
Okay, that out of the way, here are some links that I thought you’d find informative. As always, I appreciate your continued support.
• I recently lectured at the CanFitPro Conference in Toronto. While there, I got a chance to record a few interview segments for Omar Isuf’s YouTube channel. In this segment we discuss repetition ranges for maximizing muscle hypertrophy. Give this a watch and you’ll see why Omar lives up to his nickname, King of YouTube Fitness.
• I was interviewed along with my partner-in-science, Alan Aragon, on the We Do Science Podcast. Here Alan and I discuss the complexities of nutrient timing, delving into both the science and practical applications on the topic. Bonus discussion on a related topic: whether there is any fat loss benefit to doing fasted cardio. Click on Episode #8.
• I’ve appeared numerous times on Superhuman Radio; this segment might be my favorite yet. Here I discuss whether it’s possible to gain muscle simultaneously while simultaneously losing fat. Host Carl Lanore is consistently one of the best interviewers in the biz and he again shows why by asking all the right questions. l
• My friend and colleague Tom Venuto wrote an excellent post on delayed-onset muscle soreness and its relevance to muscular gains. The article covers the science in an understandable fashion, and provides solid take-home advice.
• Speaking of Tom Venuto, he wrote what I think is the most detailed review of my book, The M.A.X. Muscle Plan. Always an honor to receive praise from a true fitness pro such as Tom.
• In case you missed it, I recently published this study showing muscle activation during the leg press at 30% 1RM to failure produced significantly lower muscle activation compared to 75% 1RM. I also wrote an accompanying blog post where I break things down into consumer-friendly language and discuss the study’s implications.
• Finally, my good friend Bret Contreras wrote this terrific article that delved into the free-weights vs. machines debate. As mentioned earlier, I will be collaborating on a study examining this topic; Bret’s post provides excellent commentary on its complexities. While you’re at it, make sure to read through the references at the end of the article; it’s patently clear research doesn’t support the claims made by certain fitness pros.
In case you’re not aware, a meta-analysis involves pooling the results of studies on a given topic to achieve clarity on the body of evidence. Here is an overview of the study with my analysis of methods and findings as well as commentary on its implications:
Inclusion Criteria
An important component of a meta-analysis is the inclusion/exclusion criteria. Simply stated, this refers to what conditions must be met for studies to be included in the analysis. For this meta-analysis, researchers required that studies had the following constraints:
• Compared a “low-carb” diet (less than 45% of calories from carbs) to a “balanced” diet (45-65% calories from carbs) that were isoenergetic (same number of calories between groups) in randomized, controlled fashion
• Comprised overweight or obese subjects
• Included macronutrient breakdowns
• Spanned at least 12 weeks in length
• Contained at least 10 subjects in each group
For statistical analysis, the low-carb diets were stratified into “high fat” (containing greater than 35% lipid) or high protein (containing greater than 20% protein). The diets were then further stratified into those where subjects were type 2 diabetics or non-diabetic. This stratification allowed for sub-analysis in a manner that helped reduce the potential confounding.
At first glance it would be fair to question the fact that “low carb” was categorized as any diet containing less than 45% of total calories. However, percentages can be misleading. The only truly relevant number here is the total grams consumed from carbohydrate. Let’s take a look at how this factored in to the included trials.
For the high-fat, non-diabetic studies there was one true ketogenic diet (4% of total calories from carbs) and the others ranged between 26-38% total calories from carbs. Given that energy intakes varied from about 1500 – 1700 calories per day, this puts total carb intake at about 97 to 161 grams/day (discounting the one true keto study). On the lower end this would put most in ketosis while on the higher end it would not. Carb intake in the high-fat diabetic studies averaged 20% of total calories, which would almost certainly translate into a ketogenic state in these subjects. The “high-protein” studies were basically all “Zone” type diets using the 40-30-30 approach. In these studies the total carb intake would have been greater than 150 grams and hence not induce ketosis. Bottom line: The “high fat” groups could fairly be classified as low-carb for the most part (at least if you pool the means of these studies) while the “high protein” groups would be more appropriately placed in a balanced category.
Overall the inclusion criteria allowed for the ability to examine an important issue on the topic, namely the effects of carb intake when total calories are kept constant. As will always happen in such situations, a number of studies that can have relevance are ultimately excluded from analysis. The extent to which this impacts results cannot be determined and the entire body of literature should always be taken into consideration when drawing evidence-based conclusions for practical application to nutritional approaches.
Analytic Specifics
A total of 19 RCTs met inclusion criteria encompassing 3209 participants. The duration of the studies spanned from 3 months to 2 years. In scrutinizing the methodology, the researchers appeared to have done a nice job collecting and analyzing data. Two different researchers were involved in the search and coding process. This serves as a double-check to help minimize the prospect of errors in data entry. They screened for various types of bias (i.e. selection, performance, detection, attrition, and reporting) and did report instances where these issues could have impacted results. The one thing I did not see mentioned was an attempt to re-code a random number of the studies to check for “coder drift” (a change in the interpretation of coding items over time). It’s unlikely that this significantly impacted results, but the possibility cannot be ruled out based on what is presented in the methods section.
Results
There were no significant differences in any of the outcomes at any of the time-points measured; weight loss was similar between all of the diets as were health-related outcomes (blood pressure, blood lipids, fasting glucose). The forest plots highlight the disparity between studies, with no trend whatsoever for superiority of one diet over another. The evidence presented suggests that when calories are equated, there is no difference in weight loss or health-related markers regardless of carbohydrate intake.
Limitations
The primary limitation of the analysis is the fact that participants did not fully adhere to prescribed macronutrient goals in a majority of trials, and adherence declined with longer time periods. Compounding matters further, self-reporting of food intake is historically inaccurate, particularly in those who are overweight and obese. Thus, the strength of evidence is compromised here, making it is difficult to formulate clear conclusions from the analysis.
On the other hand, what is reinforced from this data is just how difficult it is to stick with a diet – any diet – over the long-term. As the authors of the study point out, this is especially true in diets that exclude entire food groups such as low-carb diets (although it should be noted that adherence in the balanced diet was equally poor in the studies analyzed). With respect to weight loss, nothing is more important than dietary adherence; you can’t achieve results if you don’t follow the diet.
The other point to keep in mind is that the subjects were all overweight or obese. Thus, results cannot necessarily be generalized to a healthy, non-overweight population. Now I’d point out that those who are lean tend to be more insulin-sensitive compared to the overweight/obese, and therefore low-carb diet would seemingly have less utility for these individuals. This would be particularly true of those who are serious exercisers, as both aerobic exercise and resistance training enhance insulin sensitivity. Still, the relevance of findings to lean or athletic populations remains questionable.
Perspectives
This meta-analysis provides evidence that energy balance – not macronutrient composition – is what dictates weight loss, although findings must be interpreted with caution due to poor dietary adherence across protocols. Despite this inherent limitation, results seem to be consistent with current theory on weight loss. While ketogenic diets can be a viable approach for some, I’m aware of no evidence showing that they have a universal metabolic superiority over balanced diets provided calories and protein are equated between dietary strategies. In fact, the few studies that have investigated the topic under controlled conditions failed to show any such metabolic advantage:
• Johnston et al compared a ketogenic diet (33 g carbs) to a balanced diet (157 g carbs) in a sample of 20 sedentary overweight/obese men and women. Total protein and calorie consumption were held constant so the only thing that differed between diets was intake of carbohydrate. No differences were found in fat loss or markers of cardiovascular health. The big strength of this study was that all meals were individually prepared giving a high degree of confidence in the results. The study was limited by a duration of only 6 weeks and a small sample size.
• Soenen et al. conducted an elegant study that included four isoenergetic groups of varying protein and carb content, including groups where protein was matched but carb intake varied. The study was carried out over a 12 month period with an initial 3-month phase where subjects consumed 33% of their maintenance calories followed by a 9-month phase where subjects consumed calories at 66% of maintenance. During the initial 3-month phase the low-carb group consumed 5% of calories from carbohydrate; during the second phase carb intake increased to 25% of total calories. The average total caloric intake was not disclosed, but given the percent carb values and the fairly substantial energy restriction, it would certainly appear that the subjects were in ketosis throughout the study duration. Results? Here is a direct quote from the authors: “The study showed irrefutably, that, despite the success all-over with all four diets, the answer is that it is the relatively high-protein content per se, that supports the even greater success, and not the relatively lower carbohydrate content.”
The primary take-home message here is that there is no universal “best” diet. There is compelling evidence that higher protein intakes (at least 1.5 g/kg and generally higher in those who are lifting weights) are beneficial for optimizing body composition and enhancing satiety. A certain amount of dietary lipid is also essential for proper health, particularly with respect to polyunsaturated fats. Otherwise your approach to nutrition is largely an individual choice that, within fairly wide limits, should be based on preference, goals and lifestyle. Most importantly, calories do count!
References
Naude CE, Schoonees A, Senekal M, Young T, Garner P, Volmink J. Low Carbohydrate versus Isoenergetic Balanced Diets for Reducing Weight and Cardiovascular Risk: A Systematic Review and Meta-Analysis. PLoS One. 2014 Jul 9;9(7):e100652
Johnston CS, Tjonn SL, Swan PD, White A, Hutchins H, Sears B. Ketogenic low-carbohydrate diets have no metabolic advantage over nonketogenic low-carbohydrate diets. Am J Clin Nutr. 2006 May;83(5):1055-61
Soenen S, Bonomi AG, Lemmens SG, Scholte J, Thijssen MA, van Berkum F, Westerterp-Plantenga MS. Relatively high-protein or ‘low-carb’ energy-restricted diets for body weight loss and body weight maintenance? Physiol Behav. 2012 Oct 10;107(3):374-80
A new research study on protein overfeeding is causing a bit of a stir in the fitness community. The study in question, authored by Dr. Jose Antonio et al, evaluated body composition changes in a group of men and women that consumed an additional 800 calories of protein each day (to the tune of more than 5 times the daily RDA for protein!) versus a group consuming a maintenance diet. Here is a brief rundown of the methodology and findings.
A total of 30 resistance-trained subjects (and these subjects would be considered highly trained, with an average lifting experience of almost 9 years) participated in the study: 10 in the control group who were at caloric maintenance, and 20 in the experimental group who ate a caloric surplus, with virtually all of the additional calories consumed in the form of a whey/casein protein powder. Subjects were instructed to maintain their normal resistance training programs, which were not supervised by the researchers. Total calories and macronutrient intake were calculated by self-reported daily food diaries. Body composition was assessed by a BodPod, which uses air displacement plethysmography to estimate fat mass (FM) and fat-free mass (FFM).
After 8 weeks, no statistically significant differences were seen from baseline levels in either group. That said, the high protein group did gain an average of 1.7 kg (3.7 lbs), all in the form of FFM. The food diaries indicated that subjects adhered to the diets as specified by the protocol, and the self-reported volume of training over the course of the study did not change from pre-study levels.
So what’s the controversy here? Well, some have questioned the study’s validity, claiming results violate the First Law of Thermodynamics (i.e. energy is neither created nor destroyed, but rather changed from one form to another). When extrapolated to nutrition, the First Law of Thermodynamics essentially states that the difference between calories ingested versus calories expended will dictate whether weight is gained or lost. Since the subjects in the high-protein group consumed 800 calories over maintenance, it would stand to reason that the subjects who overate should have gained a fairly extensive amount of weight. Using the generally accepted formula that 3500 equates to one pound of fat (which is a fundamentally flawed concept, but that’s a post for another day), total weight gain should have been somewhere in the range of 12 pounds over the course of the 8-week study period.
A closer look at the evidence, however, shows that the results were generally consistent with thermodynamic principles. Here’s why.
First, the thermic effect of food (TEF) for protein is very high. Simply stated, the TEF refers to the amount of calories expended in the digestion and absorption process. Protein has a much higher TEF than the other macronutrients, equating to approximately 30% of total calories. Thus, if you overeat 800 calories of protein, about 240 of these calories will be lost to thermogenesis.
Moreover, overeating results in an increase in a phenomenon called non-exercise activity thermogenesis (NEAT). As the name implies, NEAT refers to the energy expended during everything other than regimented exercise (i.e. fidgeting, maintenance of posture, activities of daily living, etc). A classic study by Levine et al found that subjects who were overfed 1000 calories a day compensated by increasing NEAT by a daily average of ~350 calories. Assuming a somewhat similar response in the Antonio et al study, this would mean that approximately 600 of the 800 extra calories consumed would have been expended via TEF and NEAT.
So we’re left to account for about 200 extra calories a day. Well, it just so happens that the reported weight gain of just over 3 pounds explains this away very nicely. The most interesting thing here is that all of the added weight was attributed to gains in FFM as opposed to body fat. This suggests that overfeeding protein well above levels normally thought to maintain a positive nitrogen balance may in fact have a small effect on enhancing the hypertrophic response to resistance training. Although the study did not provide any insight into potential mechanisms, one possibility is that very high protein intakes may help to suppress protein breakdown. Given that increases in hypertrophy are the result of the difference between protein synthesis and degradation, this hypothesis warrants further study.
I’ve heard a number of people criticize the fact that caloric intake was assessed by self-report. To this end, research does in fact show that self-reported food intake can be quite inaccurate. While certainly this is a valid concern, it should be noted that subjects in the high-protein group reported their dietary intake prior to the study as well as during the intervention. It seems logical to think that if these subjects misreported caloric intake during the study, they also would have done so to a similar extent when reporting their baseline intake. Thus, the net effect would seemingly be a fairly accurate representation of the extra calories consumed over the study period. So while there could be issues related to over-reporting of food intake, the results would seem to suggest that the factors I mentioned above are a more likely explanation.
Bottom line: The study, while intriguing, really serves as pilot data for future exploration into the topic. A big issue here is that the resistance training component was not supervised by the researchers. Thus, there is no way to verify what was actually done by the subjects and, importantly, how hard they actually trained. From what I understand, a follow-up study is already in the works that will address this issue. In the meantime, the take-home message here seems to be that if you intend to overeat (and care about your body composition), make sure the extra calories come from protein-rich foods.
Several months ago I wrote a blog post called A Dozen Must-Read Fitness Blogs. The post highlighted a number of blogs that I felt consistently put out great content on exercise and sports nutrition.
Recently, someone commented on the post asking why I didn’t include any blogs written by women. Hadn’t considered this point, but after giving it some thought I realized she was right! It was an oversight that needed to be addressed. Not that gender should make a difference when reading a blog — it’s the quality of course that counts regardless of who writes the post — but it’s nevertheless necessary to give credit where credit is due. Importantly, resistance training for women is an area that is still under-appreciated; the more we can do to make gals realize they need to embrace the iron, the better.
So I’m dedicating this post to feature some truly terrific female fitness pros and their respective blogs. When it comes to fitness, these gals get it. They’re not out there preaching that women should do endless reps with pink dumbbells and follow starvation diets. Quite the opposite, actually. They each have their own niche, but their philosophies are grounded in science and supplemented with a whole lot of good-old-fashioned in-the-trenches experience.
So without further ado, and in no particular, here are five must-read fitness blogs written by women for women (although most guys can certainly pick up a few pointers here as well). As with my previous post, this is by no means a comprehensive list. There are certainly a large number of other female bloggers that I’ve no doubt excluded and will look to cover in a follow-up blog.
• Jen Sinkler: Jen is a former rugby player turned fitness editor. She recently gave up her gig as the head honcho at Experience Life magazine to freelance at a number of the major women’s fitness mags and train clients one-on-one. Her blog is decidedly no-fluff. She focuses primarily on the performance-based aspects of lifting as opposed to training for aesthetics (although the two are not mutually exclusive). Articles are eclectic and range from areas as diverse as kettlebells to cycle circuits to biofeedback. Lots of good stuff.
• Molly Galbraith: Besides being one of the most down-to-earth individuals you’d ever want to meet, Molly is a true fitness pro. She was co-owner of a gym with Jim Laird where she specialized in working with female clients before recently stepping away to pursue online coaching and focus on maintaining her blog. Although the blog delves into a number of fitness topics, Molly’s focus is on helping women with body image issues. Her blogs are often very personal as she writes about her own struggles with body image and her journey to self-satisfaction through fitness. Moly is also co-founder of another excellent female-oriented blog, Girls Gone Strong that should be bookmarked for reading.
• Lift Like A Girl: This blog is written by Nia Shanks. Nia has a degree in exercise science and her in-depth knowledge of resistance exercise shows in her writings. Nia’s focus is on time-efficient workouts, particularly involving strength-based heavy-lifting routines. She covers aspects related to programming, technique and mindset. Some good nutritional articles as well. Lots of interesting reading. Make sure to watch her moonwalk!
• Flawless Fitness: This is Melody Schoenfeld’s blog. Full disclosure: Melody is in fact my sister. But before you claim nepotism, give her blog a read. Melody got her start as a trainer working in my gym back in the 90’s, then moved out to California to open her own facility. She tips the scales about 100 pounds but can out-lift a lot of guys (she holds several state powerlifting records). Her blog covers a wide range of topics. She’s big on kettlebells and holds certs as a master KB instructor. But she also gets into some cool alternative tools such as Indian clubs and even a medieval fighting implement called a mace.
• Stumptuous.com: This is Krista Scott Dixon’s blog. Krista can stake claim to being the original hard-core female fitness blogger and no doubt inspired many of the women on this list. She was churning out cutting-edge fitness articles around the turn of the century, telling women they should be squatting instead of performing a gazillion leg lifts. Her no-nonsense tone is refreshing, and she’s got a great sense of humor that makes her posts fun to read. Unfortunately, it seems Krista doesn’t post much anymore. The good news is that there is a ton of content on her blog that will keep you busy reading for weeks.
Writing a book is a lengthy, arduous process. To do it right involves a great deal of planning. You need to map out everything that needs to be covered and decide on the best way to organize this information into a cohesive, readable format. A diligent author spends countless hours contemplating these complexities before a single word makes it to the page. But no matter how attentive you are to detail, there are always some things you somehow miss that ultimately become apparent once the book is released. The best you can do at this point is to address any omissions ex post facto.
Based on reader feedback and questions, it has come to light that I made such an omission in my book, The M.A.X. Muscle Plan, with respect to warming up prior to training. In retrospect, this is not something that I should have taken for granted. A warm-up heightens blood flow to muscles, enhances speed of nerve impulses, increases energy substrate delivery to working muscles as well oxygen release from hemoglobin and myoglobin, and reduces the activation of energy for cellular reactions and muscle viscosity (Thacker et al. 2004). Suffice to say, it’s an important component of a workout. This post therefore will seek to rectify the oversight and address my recommendedations for the M.A.X. Muscle warm-up.
A warm-up can be divided into two distinct components: general and specific. The general warm-up – which involves performing a brief bout of low-intensity, large muscle group aerobic-type exercise – should be included in all three M.A.X. Muscle mesocycles (i.e. strength, metabolic conditioning, and hypertrophy). The purpose of the general warm-up is to elevate core temperature and increase blood flow. This has implications not only for injury prevention, but for performance as well. In fact, there is evidence that combining a general warm-up with a specific warm-up increases maximal strength to a greater degree than peforming a specific warm-up alone (Abad et al. 2011).
Virtually any cardiovascular activity can be used for the general warm-up. Modalities such as the stationary bike, stair climber, or treadmill are fine, as are most calisthenic-type exercises (such as jumping jacks, high steps). Choose whatever activity you desire as long as the basic objective is met.
As previously noted, the intensity for the general warm-up should be low. To gauge intensity, I like to use a rating of perceived exertion (RPE) scale. My preference is the Category-Ratio RPE Scale, which grades perceived effort on a range of 0-10 (where 0 is lying on your couch and 10 is an all-out sprint). Aim for an RPE of around 5, which for most would be a moderate walk or slow jog. Five to ten minutes is all you need – just enough to break a light sweat. Your resources should not be taxed, nor should you feel tired or out of breath either during or after performance. If so, cut back on the intensity. Remember, the goal here is merely to warm your body tissues and accelerate blood flow — not to achieve cardiovascular benefits or reduce body fat.
The specific warm-up augments the general warm-up. It serves to enhance neuromuscular efficiency in performing a given exercise. To optimize benefits, the exercises used in the specific warm-up should be as similar as possible to the actual activities in the workout. For example, if you are going to perform a bench press, then the specific warm-up would ideally involve performance of light sets of bench presses. In this way, the neuromuscular system gets to “rehearse” the movement before it is performed higher levels of intensity. Specific warm-up sets should always be stopped well short of fatigue – the focus here is to facilitate performance of the heavier sets.
For the M.A.X Strength Phase, I recommend at least a couple of specific warm-up sets per exercise. Since this phase employs a total body routine with very heavy loads (>85% 1RM), it is important that each exercise include specific warm-up sets. As a general rule the first set should be performed at ~40-50% of 1RM and the second set at ~60-70% 1RM. Eight to ten reps is all that is needed in these sets –any more than this is superfluous. Thereafter, you’re then ready to plow into your working sets.
For the M.A.X Hypertrophy Phase, I recommend performing a specific warm-up prior to the first exercise for each muscle group only. Since this is a split-routine where multiple exercises are performed per body part, the benefits achieved from the specific warm-up on the intial movement will carry over to the other exercises for the subsequent exercises for that muscle group. Additional warm-up sets can actually be detrimental since they can hinder generation of metabolic stress, which is a desired outcome in this phase.
Specific warm-up sets are not necessary in the M.A.X Metabolic Phase. In this phase you’re already using light weights and the initial repetitions of each working set therefore serve as “rehearsal” reps. What’s more, performance of warm-up sets is counterproductive to the goal of maximizing training density to bring about desired metabolic adaptations.
Hopefully this addresses the feedback and questions I’ve received on the topic. I’ll look to cover some additional questions I’ve received in future posts. In the meantime, keep the comments coming!
Brad
References
Abad CC, Prado ML, Ugrinowitsch C, Tricoli V, Barroso R. Combination of general and specific warm-ups improves leg-press one repetition maximum compared with specific warm-up in trained individuals. J Strength Cond Res. 2011 Aug;25(8):2242-5.
Thacker SB, Gilchrist J, Stroup DF, Kimsey CD Jr. The impact of stretching on sports injury risk: a systematic review of the literature. Med Sci Sports Exerc. 2004 Mar;36(3):371-8
Antioxidant supplements continue to be touted by many fitness professionals as a nutritional panacea. In case you’re not aware, antioxidants are the body’s scavengers. They help to defend against damage caused by reactive oxygen species (ROS) — unstable molecules that can injure healthy cells and tissues — which are produced in abundance each day during the normal course of respiration. The main culprit: oxygen. Every time you breathe, oxygen uptake causes ROS production. Environmental factors such as pollutants, smoke and certain chemicals also contribute to their formation. Their production have been linked to a multitude of ailments including arthritis, cardiovascular disease, dementia and cancer. Not surprisingly, exercise is associated with substantially greater ROS production given that it substantially inreases oxygen consumption. This has led to the supposition that antioxidant supplements are especially beneficial for hardcore exercisers.
Here’s a short-course in how the process works: Your body is made up of billions of cells held together by a series of electronic bonds. These bonds are arranged in pairs so that one electron balances the other. However, in response to various occurrences (such as oxygen consumption), a molecule can lose one of its electron pairs making it an unstable free radical. The free radical then tries to replace its lost electron by stealing one from another molecule. This sets up a chain reaction where the second molecule becomes a free radical and destabilizes a third molecule, which becomes a free radical and destabilizes a fourth molecule and so on.
To prevent rampant ROS production, your body has a sophisticated internal antioxidant system. Various antioxidant enzymes combine with antioxidants from the foods you eat to help keep ROS at bay. There are dozens of known antioxidants including Vitamin C, Vitamin E, coenzyme Q10, alpha-lipoic acid, and carotenoids, amongst others. Although these nutrients are readily obtainable from food sources, it is often postulated that it’s virtually impossible to consume adequate quantities from your daily diet, thus making supplementation mandatory. In theory, supplementing with antioxidants would seemingly make sense since a greater availability should allow for greater protection against ROS. Question is, does theory translate into practice?
I first became interested about the topic a dozen or so years ago. A friend gave me a book to read called The Antioxidant Miracle, which as the title implies touted the wonders of antioxidant supplementation. The book piqued my curiousity. I delved into the research. Lo and behold, the claims seemed legit. A large number of studies showed positive effects of supplementation on a wide array of health-related benefits. What really caught my attention was a review by Dekkers et al. in the journal Sports Medicine, which discussed favorable results of antioxidant supplements during intense physical activity. The article went on to conclude that “human studies reviewed indicate that antioxidant vitamin supplementation can be recommended to individuals performing regular heavy exercise.” At the time, I wasn’t very savvy as to the complexities of research. I jumped on the antioxidant supplement bandwagon.
My bad.
Fast forward several years. Larger randomized controlled trials were conducted. The findings of these studies were at best decidedly mixed, with a majority showing no health-related benefits from supplementing with antioxidants. Alarmingly, several meta-analyses reported that there may even be an increased supplement-associated risk for cancer, stroke, and all-cause mortality. An objective evaluation of the current literature would make it difficult for even the most ardent antioxidant proponent to make a case for improving well-being by supplementation.
What’s particularly interesting to me as an exercise scientist is emerging research suggesting that antioxidant supplements may actually have a *detrimental* effect on training-related adaptations, particularly those associated with muscle hypertrophy. At issue here is the distinction between chronic versus acute ROS production. Evidence does show that chronically elevated levels of ROS can impair muscle function and even bring about muscle wasting conditions. Understand, however, that exercise upregulates the body’s antioxidant defenses. This ultimately helps to reduce chronic elevations in ROS without the need for supplementation.
On the other hand, acute production of ROS during a workout has been implicated in a variety of exercise-related adaptations including enhanced muscle remodeling. ROS production has been found to promote growth in both smooth muscle and cardiac muscle, lending credence to the supposition that these substances may have similar hypertrophic effects on skeletal muscle as well. The mechanisms have yet to be determined, but studies show that ROS can function as key cellular anabolic signaling molecules in the response to exercise. What’s more, there is evidence that they help to mediate the activity of satellite cells, which are responsible for aiding in repair and regeneration of muscle fibers. I have covered these topics extensively in my recent reviews of the roles of metabolic stress and muscle damage in exercise-induced muscle hypertrophy. By suppressing ROS production, antioxidant supplements may inhibit these hypertrophic effects and thus impair the growth and repair process. Indeed, preliminary studies indicate a negative impact of supplementation on exercise-induced adaptations.
There are a couple of take-home messages here, the most obvious of which is that the risk/reward ratio for antioxidant supplementation appears to be poor. Focus on eating a diet replete in vegetables and fruits and you’ll get all the antioxidants you need to support basic health. Overloading on antioxidants via supplements will not confer any additional benefits; it’s possible they may actually cause harm. And although the jury is still out, it is at least conceivable that supplementation can impede muscular development and other exercise-related adaptations. Any way you slice it, antioxidant supplementation doesn’t seem to make sense, at least for otherwise healthy individuals who exercise on a regular basis.
On a broader scale, the overriding message to be gleaned is the importance of using caution when interpreting research. This is particularly true of exercise-related studies, which are usually limited by small sample sizes, the inability to control for various confounders, and the almost unlimited number of variations that encompass exercise program design. All-too-often fitness professionals are quick to form opinions based on limited evidence. Such an approach is decidedly misguided and unscientific. As illustrated here, I was guilty of falling into this trap. Fortunately I learned from the mistake and as a result became a more astute fitness professional.
Extrapolating research findings in an evidence-based fashion can be equated to solving a jigsaw puzzle. Each published study is a piece to the puzzle. In almost every situation there will be conflicting results between studies. Sometimes two studies will report diametrically opposite findings on the same topic. How can you make sense of all this?
The best fitness professionals, guys like Bret Contreras, Alan Aragon, Joe Dowdell, and James Krieger, will weigh the body of evidence by considering factors such as the type of study (experimental vs. observational), the subjects (animal vs. human), and the setting (in vitro, ex vivo, in vivo, etc). They’ll also take into account numerous other factors including study design, statistical power, generalizability, and the quality of the journal in which the study was published. Only after a thorough analysis of the prevailing body of literature can an educated opinion be formed that guides decision-making and provides the basis for practical recommendations. It’s a skill that can be honed. The more research you read, the better you become at critical thinking, allowing you to piece together the puzzle in question.
One last thing: I frequently hear trainers and even researchers cite a study as “proof” of a given opinion. Not! A single study never “proves” anything. Rather, it simply lends support to a given theory. As noted, some studies carry more weight than others. The greater the strength of evidence, the more support there is for the theory. But theories are not set in stone. Case in point: Until recently, it was taken as gospel that saturated fat and cholesterol caused cardiovascular disease. Every nutrition text, bar none, stated such as fact. Recent research has now challenged these assumptions, however, suggesting that any relationship is far more complex than previously thought. Bottom line is that the more knowledge we acquire, the more we realize just how much more there is to learn.
Always be skeptical. Always be willing to change your opinion based on new information. This is what separates the ordinary practitioners from the elite.








 Entries (RSS)
Entries (RSS)



